Download
1 / 1
10 likes | 131 Views
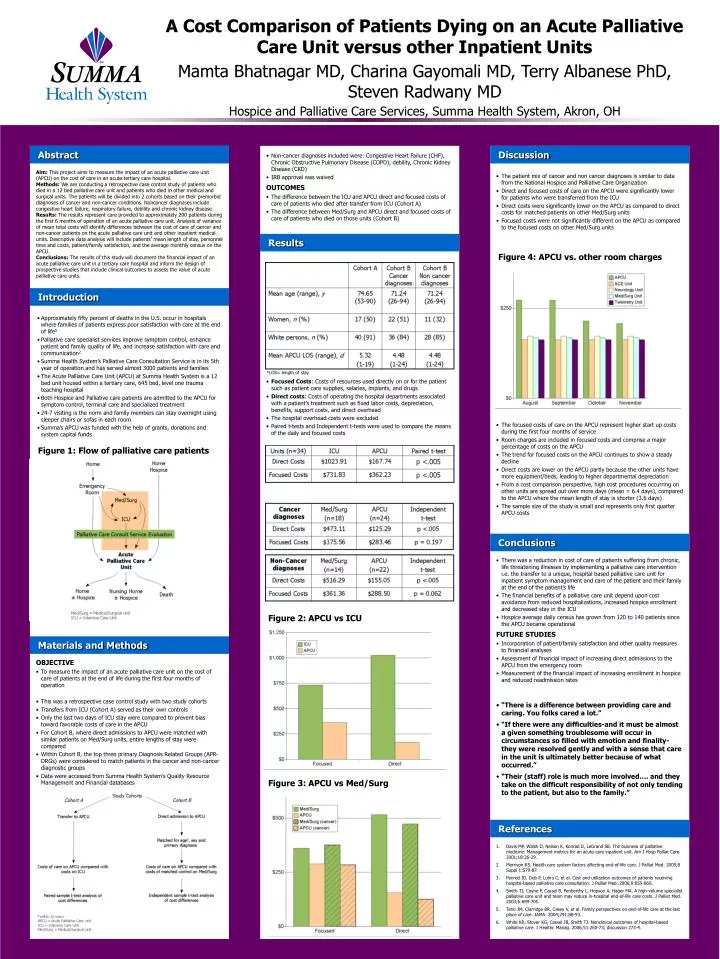
A Cost Comparison of Patients Dying on an Acute Palliative Care Unit versus other Inpatient Units. Mamta Bhatnagar MD, Charina Gayomali MD, Terry Albanese PhD, Steven Radwany MD Hospice and Palliative Care Services, Summa Health System, Akron, OH. Abstract.

E N D
A Cost Comparison of Patients Dying on an Acute Palliative Care Unit versus other Inpatient Units Mamta Bhatnagar MD, Charina Gayomali MD, Terry Albanese PhD, Steven Radwany MD Hospice and Palliative Care Services, Summa Health System, Akron, OH Abstract • Non-cancer diagnoses included were: Congestive Heart Failure (CHF), Chronic Obstructive Pulmonary Disease (COPD), debility, Chronic Kidney Disease (CKD) • IRB approval was waived • OUTCOMES • The difference between the ICU and APCU direct and focused costs of care of patients who died after transfer from ICU (Cohort A) • The difference between Med/Surg and APCU direct and focused costs of care of patients who died on those units (Cohort B) Discussion Aim: This project aims to measure the impact of an acute palliative care unit (APCU) on the cost of care in an acute tertiary care hospital. Methods: We are conducting a retrospective case control study of patients who died in a 12 bed palliative care unit and patients who died in other medical and surgical units. The patients will be divided into 2 cohorts based on their premorbid diagnoses of cancer and non-cancer conditions. Noncancer diagnoses include congestive heart failure, respiratory failure, debility and chronic kidney disease. Results: The results represent care provided to approximately 200 patients during the first 6 months of operation of an acute palliative care unit. Analysis of variance of mean total costs will identify differences between the cost of care of cancer and non-cancer patients on the acute palliative care unit and other inpatient medical units. Descriptive data analysis will include patients’ mean length of stay, personnel time and costs, patient/family satisfaction, and the average monthly census on the APCU. Conclusions: The results of this study will document the financial impact of an acute palliative care unit in a tertiary care hospital and inform the design of prospective studies that include clinical outcomes to assess the value of acute palliative care units. • The patient mix of cancer and non cancer diagnoses is similar to data from the National Hospice and Palliative Care Organization • Direct and focused costs of care on the APCU were significantly lower for patients who were transferred from the ICU • Direct costs were significantly lower on the APCU as compared to direct costs for matched patients on other Med/Surg units • Focused costs were not significantly different on the APCU as compared to the focused costs on other Med/Surg units Results Figure 4: APCU vs. other room charges Introduction • Approximately fifty percent of deaths in the U.S. occur in hospitals where families of patients express poor satisfaction with care at the end of life5 • Palliative care specialist services improve symptom control, enhance patient and family quality of life, and increase satisfaction with care and communication2 • Summa Health System’s Palliative Care Consultation Service is in its 5th year of operation and has served almost 3000 patients and families • The Acute Palliative Care Unit (APCU) at Summa Health System is a 12 bed unit housed within a tertiary care, 645 bed, level one trauma teaching hospital • Both Hospice and Palliative care patients are admitted to the APCU for symptom control, terminal care and specialized treatment • 24-7 visiting is the norm and family members can stay overnight using sleeper chairs or sofas in each room • Summa’s APCU was funded with the help of grants, donations and system capital funds *LOS= length of stay • Focused Costs: Costs of resources used directly on or for the patient such as patient care supplies, salaries, implants, and drugs • Direct costs: Costs of operating the hospital departments associated with a patient’s treatment such as fixed labor costs, depreciation, benefits, support costs, and direct overhead • The hospital overhead costs were excluded • Paired t-tests and Independent t-tests were used to compare the means of the daily and focused costs • The focused costs of care on the APCU represent higher start up costs during the first four months of service • Room charges are included in focused costs and comprise a major percentage of costs on the APCU • The trend for focused costs on the APCU continues to show a steady decline • Direct costs are lower on the APCU partly because the other units have more equipment/beds, leading to higher departmental depreciation • From a cost comparison perspective, high cost procedures occurring on other units are spread out over more days (mean = 6.4 days), compared to the APCU where the mean length of stay is shorter (3.6 days) • The sample size of the study is small and represents only first quarter APCU costs Figure 1: Flow of palliative care patients Conclusions • There was a reduction in cost of care of patients suffering from chronic, life threatening illnesses by implementing a palliative care intervention i.e. the transfer to a unique, hospital based palliative care unit for inpatient symptom management and care of the patient and their family at the end of the patient’s life • The financial benefits of a palliative care unit depend upon cost avoidance from reduced hospitalizations, increased hospice enrollment and decreased stay in the ICU • Hospice average daily census has grown from 120 to 140 patients since the APCU became operational • FUTURE STUDIES • Incorporation of patient/family satisfaction and other quality measures to financial analyses • Assessment of financial impact of increasing direct admissions to the APCU from the emergency room • Measurement of the financial impact of increasing enrollment in hospice and reduced readmission rates Figure 2: APCU vs ICU Materials and Methods • OBJECTIVE • To measure the impact of an acute palliative care unit on the cost of care of patients at the end of life during the first four months of operation • This was a retrospective case control study with two study cohorts • Transfers from ICU (Cohort A) served as their own controls • Only the last two days of ICU stay were compared to prevent bias toward favorable costs of care in the APCU • For Cohort B, where direct admissions to APCU were matched with similar patients on Med/Surg units, entire lengths of stay were compared • Within Cohort B, the top three primary Diagnosis Related Groups (APR-DRGs) were considered to match patients in the cancer and non-cancer diagnostic groups • Data were accessed from Summa Health System’s Quality Resource Management and Financial databases • “There is a difference between providing care and caring. You folks cared a lot.” • “If there were any difficulties-and it must be almost a given something troublesome will occur in circumstances so filled with emotion and finality-they were resolved gently and with a sense that care in the unit is ultimately better because of what occurred.” • “Their (staff) role is much more involved…. and they take on the difficult responsibility of not only tending to the patient, but also to the family.” Figure 3: APCU vs Med/Surg References • Davis MP, Walsh D, Nelson K, Konrad D, LeGrand SB. The business of palliative medicine: Management metrics for an acute-care inpatient unit. Am J Hosp Palliat Care. 2001;18:26-29. • Morrison RS. Health care system factors affecting end-of-life care. J Palliat Med. 2005;8 Suppl 1:S79-87. • Penrod JD, Deb P, Luhrs C, et al. Cost and utilization outcomes of patients receiving hospital-based palliative care consultation. J Palliat Med. 2006;9:855-860. • Smith TJ, Coyne P, Cassel B, Penberthy L, Hopson A, Hager MA. A high-volume specialist palliative care unit and team may reduce in-hospital end-of-life care costs. J Palliat Med. 2003;6:699-705. • Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. JAMA. 2004;291:88-93. • White KR, Stover KG, Cassel JB, Smith TJ. Nonclinical outcomes of hospital-based palliative care. J Healthc Manag. 2006;51:260-73; discussion 273-4.