Download
1 / 32
330 likes | 604 Views
OTA II. Physical Dysfunction and Activities of Daily Living: Assessment, Analysis and Intervention. Class Outline. Defining Physical Dysfunction Causes of physical dysfunction Arthritic Diseases Hip/Knee Replacements Cardiopulmonary Diseases Lab Activity. Physical Dysfunction.

E N D
OTA II Physical Dysfunction and Activities of Daily Living: Assessment, Analysis and Intervention
Class Outline • Defining Physical Dysfunction • Causes of physical dysfunction • Arthritic Diseases • Hip/Knee Replacements • Cardiopulmonary Diseases • Lab Activity
Physical Dysfunction • What is physical dysfunction? • Related to function of body structures • Strength • Muscle strength related to ability to perform Occupations and ADLs • Range of Motion • Ability to use all joints, or necessary joints for functional movement • Endurance • Ability to sustain movement over time, to enable performance of functional activity
Causes of Physical Dysfunction • Congenital • Present at birth • Examples: Cerebral Palsy, Muscular Dystrophy • Acquired • Disease • Examples: Rheumatoid arthritis, heart disease • Accidental • Examples: Hip fracture, spinal cord injury
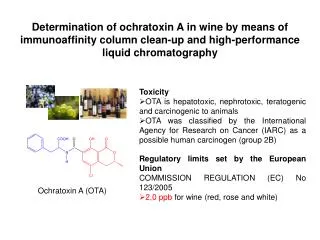
Arthritic Diseases • Osteoarthritis • Degenerative Joint Disease • Breakdown of cartilage in the joints • Rheumatoid Arthritis • Chronic, systemic autoimmune disorder • Immune system attacks the body • Leads to breakdown of joints and calcification • Gout • Metabolic disease marked by urate • Causes acute recurrent episodes of arthritis
Common Hand Deformities • Crepitation: Grating, crunching or popping sensation/sound in the joints (OA & RA) • OsteoArthritis: Osteophyte formation (Bony spur that forms along a joint) • Bouchard’s Nodes (PIP joint) • Heberden’s nodes (DIP joint)
Common Hand Deformities: Rheumatoid Arthritis • Fusiform Swelling • Swan Neck
Common Hand Deformities: Rheumatoid Arthritis • Boutonniere Deformity • Trigger Finger
Rheumatoid Arthritis Common Hand Deformities • Ulnar Drift
Rheumatoid Arthritis Common Hand Deformities • Thumb Deformities (Figure 30-9, pg. 566) • IP hyperextension, MPC flexion (most common) • IP hyperextension, MPC flexion, carpometacarpal subluxation • IP flexion, MPC hyperextention, carpometacarpal subluxation
Treatment Objectives • General objectives might include: • Maintain or increase joint mobility and strength • Increase physical endurance • Prevent, correct or minimize the effect of deformities • Maintain or increase ability to perform ADL’s • Increase knowledge about the disease and the best methods of dealing with the physical, psychological and functional effects • Assist with stress management and adjustment to physical disability.
Treatment Methods • Medical Management • Drug Therapy • Surgical • Rest • Positioning (to prevent contractures) • Physical Agent Modalities • Therapeutic Activity and Exercise (ROM exercises pg. 579 • Splinting – pg. 573 Early • support the joint in an optimal position for function and to reduce inflammation by providing rest and support to the joint • Energy Conservation (See principles of energy conservation pg. 575) • Assistive Devices (See Assistive Devices Table pg. 577) • Joint Protection • Respect pain • Maintain muscle strength and joint ROM • Avoid positions that put stress on involved joints
Hip and Knee Replacements • Weight Bearing Restrictions • NWB (Non-weight bearing) • TTWB (Toe-touch weight bearing) • PWB (Partial weight bearing) • WBAT (Weight bearing as tolerated) • FWB (Full weight bearing) • Hip Replacement Precautions • See handout
In Class Activity • Consider activity limitations with hip and knee replacements • Don’t forget precautions! • Activity Limitations • Dressing • Mobility (sit to stand transfers, driving) • Bathing and Toileting • Meal Prep and Housekeeping
Cardiac Diseases • Cardio-Obstructive Pulmonary Disease • Angina • Heart Attack (Myocardial Infarction) • Congestive Heart Failure
Cardiac Rehabilitation • Acute, inpatient rehabilitation consists of: • monitored ADL’s • instruction in cardiac and postsurgical precautions • energy conservation • graded activity • risk factor management • discharge activities • Tools for measuring a client’s response to activity are used to evaluate the cardiovascular system’s response to work. Going beyond the physician recommended maximums can put the client at risk.
Typical Cardio Measures • Heart Rate • Measured in Beats per minute • Heart rate should rise in response to activity but moderate activity should not result in maximal heart rate (could indicate need to grade the activity to conserve energy) • Blood Pressure • Pressure the blood exerts against the artery walls as the heart beats. • Rate Pressure Product • Rise at peak return to baseline in recovery • RPP = HR(beats/min) xSystolicBP • 100
OT Evaluation of Persons with Cardiopulmonary Dysfunction • Review of Medical Record (Look For): • Diagnosis • Severity • Associated Conditions • Secondary Diagnoses • Social History • Test Results • Precautions
OT Evaluation of Persons with Cardiopulmonary Dysfunction • Client Interview: • Clients with a history of angina should be asked to describe in terms of intensity of episodes, and if they’ve had a MI can they differentiate between the symptoms • Identify activities that bring shortness of breath • Look For • Signs of Anxiety • Shortness of Breath • Confusion • Difficulty comprehending • Fatigue • Posture • Endurance • Ability to Move • Family Dynamics
OT Evaluation of Persons with Cardiopulmonary Dysfunction • Clinical Assessment: • Determine client’s present functional ability and limitations • Monitored for heart rate, BP and signs/symptoms of cardiac/respiratory distress during an evaluation of tolerance to postural changes, and a functional task • See Early pg. 669 table 35-2 and 673 table 35-3 • Range of Motion, Strength and sensation may be assessed. • Client’s cognitive and psychosocial status will become apparent through interview and observation. • Formal assessments only used if concerns arise
OT Treatment of Persons with Cardiopulmonary Dysfunction • Guided by present clinical status, recent functional history, response to current activity, and prognosis • Energy costs of an activity and the factors that influence them can further guide the OTA in safe progression of activity (Oxygen consumption often used) • Resting quietly in a bed requires the least amount of oxygen per kilogram of body weight • 1basal metabolic equivalent (MET) OR • 3.5ml of Oxygen/kilogram body weight
OT Treatment of Persons with Cardiopulmonary Dysfunction • As activity increases more oxygen is required to meet the demands of the task • See pg. 674 table 35-4 for MET values associated with self-care and homemaking tasks • As a general rule, once clients tolerate an activity (ex. Seated sponge bathing) with appropriate responses, they can progress to the next higher MET level activity (ex. Standing sponge bath) • Duration of activity must be considered when determining activity guidelines
OT Treatment of Persons with Cardiopulmonary Dysfunction • A person with difficulty performing a 2 MET activity must still use a commode (3.5METS) or bedpan (5METS) for their bowel management. A person can perform at a higher than usual MET level for brief periods without adverse effects.
OT Treatment of Persons with Cardiopulmonary Dysfunction • Diaphragmatic breathing: • Benefits some clients • Breathing patternt hat calls for increased use of the diaphragm to improve chest volume • Clients can learn this technique by placing a small paperback novel on the abdomen just below the thorax. The client lies supine and is instructed to inhale slowly and make the book rise. Exhalation through pursed lips should cause the book to fall.
OT Treatment of Persons with Cardiopulmonary Dysfunction • Relaxation: • Progressive muscle relaxation in conjunction with breathing exercises can be effective in decreasing anxiety and in controlling shortness of breath. • One technique involves tensing the muscle groups while slowly inhaling, followed by relaxation of the muscle groups when exhaling twice as slowly through pursed lips. • It is helpful to teach the client a sequence of muscle groups to tense and relax. One common sequence involves: • Tensing and relaxing the face • Followed by the face and neck • Next the face, neck and shoulders • Etc…. • Until you reach the toes • A calm, quiet and comfortable environment is important for learning.
OT Treatment of Persons with Cardiopulmonary Dysfunction • Energy Conservation: • Can help clients perform at a higher funcitonal level without expending more energy. • Based on knowledge of how specific factors increase the body’s workload • 6 variables that increase oxygen demands: • Increased work rate or activity pace • Increased resistance • Increase use of large muscles • Increased involvement of trunk musculature • Raising the arms • Isometric work (straining) • Arm activity has also been shown to require a greater cardiovascular output than lower extremity activity • Standing activities require more energy then seated activities.
OT Treatment of Persons with Cardiopulmonary Dysfunction • Energy Conservation Cont’d: • Extremes of temperature, high humidity, and pollution make the heart work harder • Exhaling with exertion is more energy efficient and helps control the rate of increase of systolic blood pressure with activity. • By applying all this information, suggestions can be made for modifying an activity that will decrease the amount of energy required for the task. • Should be client centred • Use of time management important
Client and Family Education: • Must be taught and reinforced to the client and family members by the team: • Pulmonary anatomy • Disease process • Symptom management • Risk factors • Diet • Exercise • Energy conservation • Including family members provides support indirectly to the client through the family unit. Such support is critical when a client is dependent on the help of a family member to accomplish everyday tasks.
Lab Activity • For the following activities think of 3 means of conserving energy, considering that you have a client with cardiac and pulmonary difficulties: • Making vegetable soup • Planting a flower garden/vegetable garden • Washing, drying and styling their hair • Starting an independent fitness program • Getting groceries • Cleaning a bathroom Please explain your choices for each one and hand this in as your lab mark for this week.