Download
1 / 32
350 likes | 429 Views
ABG Interpretation & Acid-Base Disorders. Jeremy Barnett MD ~ Department of Critical Care Amy Gutman ~ Department of Emergency Medicine. Outline. ABG analysis steps Calculating anion gap Calculating delta gap Differentials for specific acid-base disorders A-a Gradients.

E N D
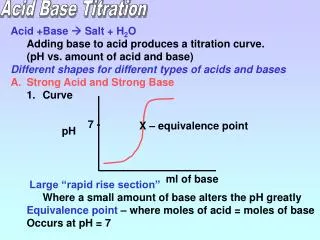
ABG Interpretation & Acid-Base Disorders Jeremy Barnett MD ~ Department of Critical Care Amy Gutman ~ Department of Emergency Medicine
Outline • ABG analysis steps • Calculating anion gap • Calculating delta gap • Differentials for specific acid-base disorders • A-a Gradients
What Are You Ordering When Requesting An ABG? PO2 PCO2 pH Electrolytes (Na+, K+, Ca++) Lactate HCO3- SaO2 Other calculated results
ABG Analysis Steps Is the pH acidemic or alkalemic? Is the primary disorder respiratory or metabolic? Is the compensation appropriate? Is the compensation acute or chronic? Is there an anion gap? If there is a anion gap, does the delta-delta indicate an additional non-anion gap? What is the differential diagnosis for the clinical process(es)?
Is Patient Hypoxic (Normal: 80-100mmHg) ? ?A-a Gradient Compensated Defect No Defect Hypoventilation Other Defect Step 1: Determine Adequacy of Oxygenation (PaO2) NO YES ?A-a Gradient NORMAL NORMAL HIGH HIGH
Step 2: Determine pH (Acidemic vs Alkalemic) • Normal pH range: 7.35–7.45 • pH <7.4 = Acidosis / increased serum hydrogen ion concentration • pH >7.4 = Alkalosis / decreased serum hydrogen ion concentration • Both metabolic & respiratory abnormalities can alter pH • Respiratory & renal function strive to keep pH = 7.4 • Minute ventilation responds quickly to metabolic acid-base problems • Renal bicarbonate excretion or retention takes days to compensate for respiratory acid-base problems • For our purposes, 3 questions: • Is abnormality respiratory or metabolic? • If respiratory, is it acute or chronic? • If metabolic, is respiratory system responding appropriately?
Step 3: Determine Primary Disorder Acidemic (pH < 7.40) Alkalemic (pH > 7.40) PCO2 PCO2 > 40mmHg < 40mmHg > 40mmHg < 40mmHg Respiratory Acidosis Metabolic Acidosis Metabolic Alkalosis Respiratory Alkalosis
Primary Disorder • If pH & PCO2 going in opposite direction = Respiratory • If pH & PCO2 going in same direction = Metabolic • May not work with mixed disorders
Step 4: Appropriate Compensation? Chronic or Acute? • Acute Respiratory Acidosis • For every 10 increase in pCO2, HCO3 increases by 1, pH decreases 0.08 • Acute Respiratory Alkalosis • For every 10 decrease in pCO2, HCO3 decreases by 2, pH increases 0.08 • Chronic Respiratory Acidosis • For every 10 increase in pCO2, HCO3 increases by 4, pH decreases 0.03 • Chronic Respiratory Alkalosis • For every 10 decrease in pCO2, HCO3 decreases by 5, pH increases 0.03 • Partial Compensation: Change in pH between 0.03 - 0.08 for every 10mmHg change in PCO2
Respiratory Component (PaCO2)? • Normal range: PaCO2 35–45 mmHg • Primary respiratory acidosis if pH <7.35 & HCO3– normal • PaCO2 >45mmHg: Respiratory compensation for metabolic alkalosis if pH >7.45 & HCO3– increased • PaCO2 <35mmHg: Primary respiratory alkalosis if pH >7.45 & HCO3– normal • Respiratory compensation for metabolic acidosis if pH <7.35 & HCO3– decreased
Metabolic Component (HCO3)? • Normal HCO3– range 22–26mmol/L • HCO3 <22mmol/L: Primary metabolic acidosis if pH <7.35 • Renal compensation for respiratory alkalosis if pH >7.45 • HCO3 >26mmol/L: Primary metabolic alkalosis if pH >7.45 • Renal compensation for respiratory acidosis if pH <7.35
Base Excess ~ Degree of Metabolic Disturbance • Bicarbonate poor indicator of acid-base disturbance as affected by respiratory & metabolic components • Base excess (-2 to +2mEq/L) • Dose of acid or alkali to return blood to normal pH • Examples: • Abnormal base excess with normal AG • Normal AG metabolic acidosis (hypercholoremia, GI HCO3 loss, RTA) • Normal base excess with abnormal AG • Lactic acidosis, HAGMA with pre-existing metabolic alkalosis • HAGMA masked by hypoalbuminemia (uncorrected AG) • ASA toxicity: respiratory alkalosis + increased AG metabolic acidosis
Appropriateness of Respiratory Response to Metabolic Acidosis Predicted Change in PCO2 = (1.5 x HCO3) + 8 If patient’s PCO2 is roughly this value, the response is appropriate If patient’s PCO2 higher than this value, they are failing to compensate
Winter’s Formula ~ Predicting pCO2 in Metabolic Acidosis Expected pCO2 = (1.5 x HCO3) + 8 + 2 In metabolic acidosis the expected pCO2 estimated from HCO3 pCO2 (actual) > pCO2 (predicted) = additional respiratory acidosis (“mixed acidosis”) pCO2 (actual) < pCO2 (predicted) = respiratory alkalosis
Step 5: Calculate Anion Gap • AG = Na+ – (HCO3- + Cl-) • Alternative: (Na+ + K) – (HCO3- + Cl-) • Normal 12 ± 2 • If albumin <4 add 2.5 to AG for every decrease of 1 • Corrected = AG + 2.5 [4 – albumin] • If no AG, evaluate for non-anion gap acidosis • If there is an AG, calculate delta gap (“excess anion gap”) • Calculate delta gap if AG to determine “hidden” metabolic disorders (i.e. non-AG metabolic acidosis, metabolic alkalosis)
Step 6: Calculate Delta Gap • Compares increase in anion gap to the decrease in HCO3 • Delta gap = (Actual AG – 12) + HCO3 • Delta gap >30 = additional metabolic alkalosis • Delta gap < 18 = additional non-gap metabolic acidosis • Delta gap 18–30 = no additional metabolic disorders
Example Delta Gap Calculation • ABG 7.23 / 17 / 235 on 50% ventimask • BMP Na 123 / Cl 97/ HCO3 7/ Albumin 4 • Delta gap = (actual AG – 12) + HCO3 = (19-12) + 7 = 14 • Delta gap <18 = Additional non-AG metabolic acidosis = Metabolic acidosis anion & non-anion gaps
Delta Ratio & Delta Gap ~ High Anion Gap Metabolic Acidosis (HAGMA) Delta Gap = (Actual AG – 12) + HCO3 Delta Ratio = AG = (AG – 12) HCO3 = (24 – HCO3) • < 0.4 Hyperchloremic Non-AG metabolic acidosis • 0.4–0.8 HAGMA + NAGMA • 1-2 Pure HAGMA • >2 Metabolic Acidosis w/ pre- existing elevated HCO3 (metabolic alkalosis or respiratory acidosis) • DG > 30 Additional metabolic alkalosis • DG < 18 Additional non-anion gap metabolic acidosis • DG 18–30 No additional metabolic disorder Evaluate if high AG metabolic acidosis
Non-Anion Gap Metabolic Acidosis • For non-AG metabolic acidosis, calculate urine anion gap • UAG = UNa+ + UK+ – UCL- • If UAG>0: renal problem • If UAG<0: non-renal problem
Osmolar Gap • Elevated osmolar gap >10 provides indirect evidence for presence of an abnormal low molecular weight solute (e.g. ethanol, methanol & ethylene glycol) • Osmolar gap = Osmolality (mOsm/kg) – Osmolarity (mOsm/L) • Osmolality is measured, Osmolarity is calculated • Osmolarity = (1.86 x Na+) + glucose + urea + 9 (mmol/l) • Osmolarity = (1.86 x Na+) + glucose/18 + BUN/2.8 + 9 (mg/dl)
Metabolic Alkalosis • Determine urinary Cl- to differentiate saline responsive vs saline resistant • Must be off diuretics in order to interpret urine chloride
Alveolar–Arterial (A-a) Gradient A-a Gradient = PAO2 – PaO2 Normal < [Age/ 4] + 4 • Measure of difference between alveolar & arterial O2 concentration • Normal = 5-10mmHg, plus age-related changes • Hypoxemia DDX by assessing integrity of alveolar capillary unit • In high altitude, arterial O2 low but only because alveolar O2 also low • In ventilation perfusion mismatch (PE, right-to-left shunt), O2 not effectively transferred from alveoli to blood resulting in elevated A-a gradient
Summary • Stepwise analysis • Clinical suspicion + labs = differential diagnosis • ABG is a set of numbers… use as part of the “big picture” not an isolated value