Download

1 / 39
390 likes | 644 Views
SAMHSA Grant Kickoff Meeting. March 14, 2012. Kickoff Meeting Agenda. 11:00-11:30 Welcome, Introductions and Roll call Polly Mullins-Bentley, Acting Executive Director, CHFS, Governor’s Office of Electronic Health Information (GOEHI)

E N D
SAMHSA Grant Kickoff Meeting March 14, 2012
Kickoff Meeting Agenda • 11:00-11:30 Welcome, Introductions and Roll call • Polly Mullins-Bentley, ActingExecutive Director, CHFS, Governor’s Office of • Electronic Health Information (GOEHI) • GOEHI/Kentucky Health Information Exchange • 11:30-12:30 SAMHSA Grant Overview • Karen Chrisman, Staff Attorney, CHFS, GOEHI • - What’s This All About? • - GOEHI SAMHSA Project Plan • - 42 CFR Consent Model • - View of Clinical Information • >Continuity of Care Document (CCD) • >NetSmart CCD • - Feedback Request • 12:30-12:35 eHealth Summit Information • 12:35-1:00 Questions and Answers
KHIE Update • Polly Mullins-Bentley, ActingExecutive Director, • CHFS, Governor’s Office of Electronic Health Information (GOEHI) • KHIE /GOEHI Overview
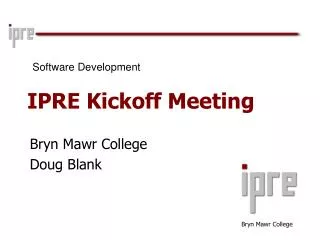
KHIE Implementation 80 Combined Hospitals/Physicians by County Updated 04/07/2011 Campbell Boone Hospital Physician Both Kenton Gallatin Bracken Pendleton Carroll Grant Mason Trimble Owen Greenup Robertson Lewis Henry Harrison Oldham Fleming Nicholas Carter Franklin Boyd Scott Shelby Rowan Bourbon Jefferson Bath Elliott Woodford Lawrence Spencer Fayette Bullitt Montgomery Anderson Menifee Clark Jessamine Meade Morgan Hancock Powell Johnson Mercer Henderson Martin Nelson Breckinridge Washington Wolfe Estill Union Daviess Madison Magoffin Hardin Garrard Boyle Lee Larue Marion Floyd Breathitt Webster McLean Pike Lincoln Ohio Jackson Owsley Grayson Rockcastle Crittenden Taylor Knott Hart Casey Perry Hopkins Edmonson Green Butler Muhlenberg Clay Livingston Caldwell Pulaski Leslie Laurel Letcher Adair Ballard McCracken Metcalfe Russell Lyon Warren Barren Carlisle Marshall Christian Knox Logan Todd Cumberland Harlan Trigg Wayne Whitley Graves Simpson Allen Hickman Clinton McCreary Monroe Bell Calloway Fulton
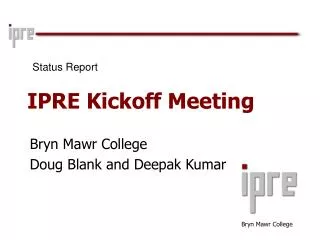
KHIE Implementation Queue 216 Combined Hospitals/Physicians/Labs/Other by County Updated 06/30/2011 Campbell Boone Hospital Physician Both Kenton Gallatin Bracken Pendleton Carroll Grant Mason Trimble Owen Greenup Robertson Lewis Henry Harrison Oldham Fleming Nicholas Carter Franklin Boyd Scott Shelby Rowan Bourbon Jefferson Bath Elliott Woodford Lawrence Spencer Fayette Bullitt Montgomery Anderson Menifee Clark Jessamine Meade Morgan Hancock Powell Johnson Mercer Henderson Martin Nelson Breckinridge Washington Wolfe Estill Union Daviess Madison Magoffin Hardin Garrard Boyle Lee Larue Marion Floyd Breathitt Webster McLean Pike Lincoln Ohio Jackson Owsley Grayson Rockcastle Crittenden Taylor Knott Hart Casey Perry Hopkins Edmonson Green Butler Muhlenberg Clay Livingston Caldwell Pulaski Leslie Laurel Letcher Adair Ballard McCracken Metcalfe Russell Lyon Warren Barren Carlisle Marshall Christian Knox Logan Todd Cumberland Harlan Trigg Wayne Whitley Graves Simpson Allen Hickman Clinton McCreary Monroe Bell Calloway Fulton
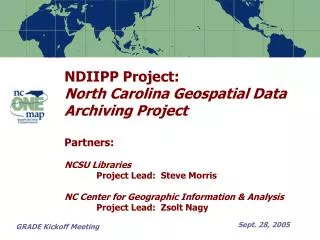
KHIE Implementation Contacts 288 Combined Hospitals/Physicians/Labs/Other by County Updated 09/28/2011 Campbell Boone Hospital Physician Both Kenton Gallatin Bracken Pendleton Carroll Grant Mason Trimble Owen Greenup Robertson Lewis Henry Harrison Oldham Fleming Nicholas Carter Franklin Boyd Scott Shelby Rowan Bourbon Jefferson Bath Elliott Woodford Lawrence Spencer Fayette Bullitt Montgomery Anderson Menifee Clark Jessamine Meade Morgan Hancock Powell Johnson Mercer Henderson Martin Nelson Breckinridge Washington Wolfe Estill Union Daviess Madison Magoffin Hardin Garrard Boyle Lee Larue Marion Floyd Breathitt Webster McLean Pike Lincoln Ohio Jackson Owsley Grayson Rockcastle Crittenden Taylor Knott Hart Casey Perry Hopkins Edmonson Green Butler Muhlenberg Clay Livingston Caldwell Pulaski Leslie Laurel Letcher Adair Ballard McCracken Metcalfe Russell Lyon Warren Barren Carlisle Marshall Christian Knox Logan Todd Cumberland Harlan Trigg Wayne Whitley Graves Simpson Allen Hickman Clinton McCreary Monroe Bell Calloway Fulton
KHIE Implementation Contacts 374 Combined Hospitals/Physicians/Labs/Other by County Updated 01/04/2012 Campbell Boone Hospital Physician Both Kenton Gallatin Bracken Pendleton Carroll Grant Mason Trimble Owen Greenup Robertson Lewis Henry Harrison Oldham Fleming Nicholas Carter Franklin Boyd Scott Shelby Rowan Bourbon Jefferson Bath Elliott Woodford Lawrence Spencer Fayette Bullitt Montgomery Anderson Menifee Clark Hancock Jessamine Meade Morgan Powell Johnson Mercer Henderson Martin Nelson Breckinridge Washington Wolfe Estill Union Daviess Madison Magoffin Hardin Garrard Boyle Lee Larue Marion Floyd Breathitt Webster McLean Pike Lincoln Ohio Jackson Owsley Grayson Rockcastle Crittenden Taylor Knott Hart Casey Perry Hopkins Edmonson Green Butler Muhlenberg Clay Livingston Caldwell Pulaski Leslie Laurel Letcher Adair Ballard McCracken Metcalfe Russell Lyon Warren Barren Carlisle Marshall Christian Knox Logan Todd Cumberland Harlan Trigg Wayne Whitley Graves Simpson Allen Hickman Clinton McCreary Monroe Bell Calloway Fulton
KHIE Implementation Contacts 483 Combined Hospitals/Physicians/Labs/Other by County Updated 03/09/2012 Campbell Boone Hospital Physician Both Kenton Gallatin Bracken Pendleton Carroll Grant Mason Trimble Owen Greenup Robertson Lewis Henry Harrison Oldham Fleming Nicholas Carter Franklin Boyd Scott Shelby Rowan Bourbon Jefferson Bath Elliott Woodford Lawrence Spencer Fayette Bullitt Montgomery Anderson Menifee Clark Hancock Jessamine Meade Morgan Powell Johnson Mercer Henderson Martin Nelson Breckinridge Washington Wolfe Estill Union Daviess Madison Magoffin Hardin Garrard Boyle Lee Larue Marion Floyd Breathitt Webster McLean Pike Lincoln Ohio Jackson Owsley Grayson Rockcastle Crittenden Taylor Knott Hart Casey Livingston Perry Hopkins Edmonson Green Butler Muhlenberg Clay Caldwell Pulaski Leslie Laurel Letcher Adair Ballard McCracken Metcalfe Russell Lyon Warren Barren Carlisle Marshall Christian Knox Logan Todd Cumberland Harlan Trigg Wayne Whitley Graves Simpson Allen Hickman Clinton McCreary Monroe Bell Calloway Fulton
KHIEA Value Added Proposition Impacting the Healthcare of Kentuckians • Use of Policy Levers • Medicaid Claims Data • KHIE was seeded with two years worth /now three years • State Laboratory Results • Microbiology LIVE since July 2011/Newborn screenings in TEST • Kentucky Immunization Registry • KHIE offers a LIVE interface for providers to report vaccinations and populate the immunization registry • Managed Care Organizations • Medicaid requires providers to connect to KHIE • Access provided to Case Managers for comprehensive case management/improved continuity of care
KHIE A Value Added Proposition • Policy Levers, continued.. • Prescription Drug Monitoring Program (KASPER) • Integration of KASPER into KHIE • Kentucky Cancer Registry • Submit cancer data for providers to the KY Cancer Registry
Participation Agreements Tracking March 12, 2012
KHIECC Coordinating Council KHIE Coordinating Council serves as an advisory body to the Governor’s Office of Electronic Health Information. Membership includes stakeholders from hospitals, physicians, mental health, public health, health insurance companies, universities and State Government representatives. The Committees include: KHIECC Accountability and Transparency KHIECC Business Development and Finance KHIECC Interoperability and Standards Development KHIECC Privacy and Security KHIECC Provider Adoption and Meaningful Use KHIECC Population Health KHIECC Clinical Advisory Committee (NEW)
“Substance abuse and its consequences have grave impacts on our society ‑‑ destroying lives, tearing apart families, and introducing drug‑related violence to our neighborhoods.” April 06, 2011 President Barack Obama
President’s Vision for Health IT Medical information will follow consumers so that they are at the center of their own care. Consumers will be able to choose physicians and hospitals based on clinical performance results made available to them. Clinicians will have a patient's complete medical history, computerized ordering systems, and electronic reminders.
President’s Vision for Health IT (cont’d) Quality initiatives will measure performance and drive quality-based competition in the industry. Public health and bioterrorism surveillance will be seamlessly integrated into care. Clinical research will be accelerated and post-marketing surveillance will be expanded.
Kathleen Sebelius Secretary U.S. Department of Health & Human Services September 29, 2009 “The increased use of health information technology is a key focus of our reform efforts because it will help to improve the safety and quality of health care generally while also cutting waste out of the system.”
The Impact of Health Reform Prior to implementation of coverage expansion under Health Reform: 39% of individuals served by State Mental Health Authorities did not have insurance 61% of the individuals served by State Substance Abuse Agencies did not have insurance Many of these individuals will be covered in 2014 (or sooner)—most likely by the expansion in Medicaid
SAMHSA’s Strategic Initiative – (Health IT) Purpose: Ensure the behavioral health provider network, including prevention specialists and consumer providers, fully participates with the general health care delivery system in the adoption of Health Information Technology. Primary role of SAMHSA’s Health IT effort is to support the behavioral health aspects of the Electronic Health Record based on the standards and systems promoted by the Office of the National Coordinator for Health IT.
SAMHSA’s Strategic Initiative “Health IT Goals” Develop the infrastructure for interoperable Electronic Health Records, including privacy, confidentiality, and data standards. Provide incentives and create tools to facilitate the adoption of Health IT and EHRs with behavioral health functionality in general and specialty healthcare settings. Deliver technical assistance to state health IT leaders, behavioral health and health providers, patients/consumers, and others to increase adoption of EHRs and health IT with behavioral health functionality. Enhance capacity for the exchange and analysis of EHR data to assess quality of care and improve patient outcomes.
IMPORTANCE OF HEALTH INFORMATION EXCHANGE (HIE) Secure information sharing between Behavioral Health Care and Primary Care Organizations; State, Federal and Other Payers. Inclusion and Reporting of Behavioral Health Data within the requirements of the State-wide Strategic and Operational Plans (Committees, Governance, & Workgroups, etc.) Infrastructure to exchange Behavioral Health and Physical Health Data using Certified EHR Systems in support of Integrated Care Delivery & Performance Reporting Interoperability – Demonstration of Behavioral Health Care Organizations participation in the Nation-wide Health Information Network (NWHIN)
SAMHSA Grant Overview • State Designated Entity Health Information Exchange Sub Awardee • Five states chosen • Kentucky • Illinois • Rhode Island • Oklahoma • Maine • Develop infrastructure supporting the exchange of health information among behavioral health and physical health providers through the development or adaptation of HIE systems
SAMHSA Grant Overview • GOEHI’s Plan • Assist the existing PBHCI recipient with KHIE connectivity • Provide connectivity for other CMHCs • Enhance the capability of the KHIE and the current CCD • Develop a 42 CFR 2 compliant consent • Develop consent training protocols • Inform both healthcare providers and consumers about this process
SAMHSA KY Plan • Kentucky HIE-SDE Sub Awardee Plan • Query based model • Consent workgroup • Interface from behavioral health providers to KHIE • Lab results reporting to behavioral health providers using KHIE as the delivery system • Training for behavioral health staff in the consent process and with the KHIE portal • Continuing education support about this program for both primary care and behavioral health providers
CCD Components • Patient: Given Name Family Name , Jr. or Sr., etc...Street Address City, State, Zip Codetel:+19995551212 MRN: 123456789 Birthdate: January 1, 1954 Sex: Male Guardian: • Next of Kin: Given Name + Family Name Street Address City, State, Zip Codetel:(999)555-1212 • Table of Contents • Purpose : Automated Medical History Summary • Payers • Problems • Family history • Social History • Allergies, Adverse Reactions, Alerts • Medications • Immunizations • Vital Signs • Results • Procedures • Encounters
Statutes and Regulations • 42 USC § 290dd-2 & 42 CFR Part 2 • The purpose of the statute and regulations prohibiting disclosure of records relating to substance abuse treatment, except with the patient's consent or a court order after good cause is shown, is to encourage patients to seek substance abuse treatment without fear that by doing so their privacy will be compromised
Statutes and Regulations • Q1. Does the federal law that protects the confidentiality of alcohol and drug abuse patient records allow information about patients with substance use disorders to be included in electronic health information exchange systems?
Statutes and Regulations • Yes. The federal confidentiality law and regulations (codified as 42 U.S.C. § 290dd-2 and 42 CFR Part 2 (“Part 2”)) permits patient information to be disclosed to Health Information Organizations (HIOs)and other health information exchange (HIE) systems. • However, the regulation contains certain requirements for the disclosure of information by substance abuse treatment programs; most notably, patient consent is required for disclosures, with some exceptions. • This consent requirement is often perceived as a barrier to the electronic exchange of health information. • It is possible to electronically exchange drug & alcohol treatment information while also meeting the requirements of Part 2.
Statutes and Regulations-Consent • Q11. What are the required elements of a patient consent under Part 2?
Statutes and Regulations-Consent • A written consent to a disclosure under the Part 2 regulations must be in writing and include all of the following items (42 CFR § 2.31): • 1) the specific name or general designation of the program or person permitted to make the disclosure; • 2) the name or title of the individual or the name of the organization to which disclosure is to be made; • 3) the name of the patient; • 4) the purpose of the disclosure; • 5) how much and what kind of information to be disclosed;
Statutes and Regulations-Consent • 6) the signature of the patient and, when required for a patient who is a minor, the signature of a person authorized to give consent under § 2.14; or, when required for a patient who is incompetent or deceased, the signature of a person authorized to sign under § 2.15 in lieu of the patient; • 7) the date on which the consent is signed; • 8) a statement that the consent is subject to revocation at any time except to the extent that the program or person which is to make the disclosure has already acted in reliance on it. Acting in reliance includes the provision of treatment services in reliance on a valid consent to disclose information to a third party payer; and • 9) the date, event or condition upon which the consent will expire if not revoked before. This data, event, or condition must insure that the consent will last no longer than reasonably necessary to serve the purpose for which it is given.
Statutes and Regulations-Consent • Q12. What must a Part 2 program do to notify the HIO, or any other recipient of Part 2 protected information, that it may not redisclose Part 2 information without patient consent? • Part 2 requires each disclosure made with written patient consent to be accompanied by a written statement that the information disclosed is protected by federal law and that the recipient cannot make any further disclosure of it unless permitted by the regulations. • Thus, when information is disclosed electronically, an accompanying notice explaining the prohibition on redisclosure must also be electronically sent.
FAQS • References for SAMHSA FAQs • http://www.samhsa.gov/healthprivacy/docs/ehr-faqs.pdf • http://www.samhsa.gov/HealthPrivacy/ • http://www.samhsa.gov/about/laws/SAMHSA_42CFRPART2FAQII_Revised.pdf
KY eHealth Summit Reminder! MARK YOUR CALENDAR! September 17 KHIECC and eHealth Network Board Joint Meeting 5:00 – 6:30 p.m. Hyatt Regency, Lexington, KY Welcome Reception 6:30 – 9:00 p.m. Hyatt Regency, Lexington, KY September 18 eHealth Summit 9:00 – 4 p.m. Invited speakers include: H. Westley Clark, M.D., J.D., M.P.H., CAS, FASAM Regional Director Center for Substance Abuse Treatment Substance Abuse Mental Health Services Administration U.S. Department of Health and Human Services Michael R. Lardiere, LCSW Vice President Health Information Technology and Strategic Development The National Council for Community Behavioral Healthcare Keynote Speaker: Kathleen Sebelius Secretary Health and Human Services
Q & A Questions and Answers Polly.Mullins-Bentley@ky.gov Karen.Chrisman@ky.gov April.Smith@ky.gov