Download
1 / 71
720 likes | 1.08k Views
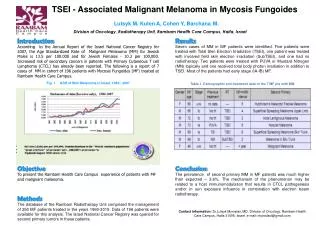
Insitu malignant melanoma. Pagetoid. spread. of malignant melanocytes (arrows). confined to. the epidermis. Lymphocytes in dermis. Invasive Malignant melanoma Mitoses –prognostic factor 3. non pigmented. pigmented.

E N D
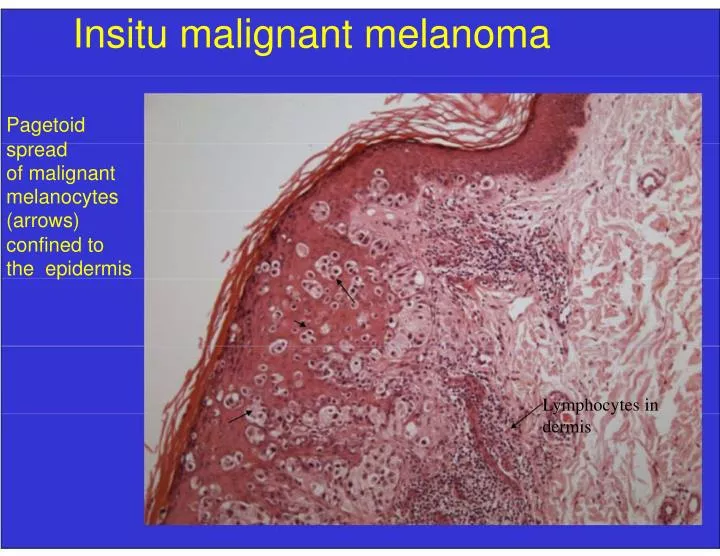
Insitu malignant melanoma Pagetoid spread of malignant melanocytes (arrows) confined to the epidermis Lymphocytes in dermis
Invasive Malignant melanoma Mitoses –prognostic factor 3 non pigmented pigmented Melanoma cells are large with round nuclei containing nucleolus Mitoses (arrow)
Ulcerated nodular melanoma Ulceration -prognostic factor 4 Ulceration
Sentinel Node Biopsy • Performed in patients with - invasive melanoma of ≥1mm Breslow thickness or Clark level IV - no clinically evident metastatic disease • +Sentinel node is the most important prognostic factor in invasive melanoma ≥1mm Breslow thickness
Sentinel node: metastatic melanoma Prognostic factor 5 Lymph node Melanoma
Melanoma- 6 Major Prognostic Factors in TNM staging • Breslow thickness • Clark level • Mitoses • Ulceration • Sentinel lymph node status • Satellite nodule (intransit metastasis) Important slide
SKIN RASHES Clinicopathologic Review Session W
How to Describe a Lesion SCALDA – Loo Very important • Size • Color • Arrangement (configuration) • Lesion morphology • Distribution • Always check hair, nail, mucosa, intertriginous areas
Arrangement (configuration) - manner in which lesions relate to one another Grouped Annular Geographic Linear SCALDA
Lesional morphology • Macule/patch: ≤/>1cm flat lesion • Papule/plaque: ≤/> 1cm raised lesion • Nodule: >1 cm raised lesion, rounded surface • Vesicle/bulla: ≤/> 1 cm blister • Surface - scale/crust/excoriated – Scale: dry/flaky surface - Crust (Scab): wet, dried serum, pus or blood - Excoriation: scratching SCALDA
Rashes for Clinicians • Dermatitis (Eczema) • Papulosquamous lesions • Vasculitis, cutaneous manifestations of systemic diseases • Drug reactions • Vesiculo-bullous diseases • Infections • Acne
Rashes - Role of a pathologist • 3-5% of lesions -difficult for clinicians -G od -O nly -K nows • Biopsy -Single Most Important Test
Biopsy Methods Excisional B Tumor Incisional B Rash Punch B Shave B
Punch biopsy 3mm 4mm 6mm
Selection of Punch Biopsy- Selection of Biopsy Rash • Biopsy early/well developed rashes • Avoid - excoriated lesions, ulcers - Burned out late lesions - Sec. infected lesions • Biopsy periphery of lesion including normal skin
Biopsy transportation BiopsyF ixatives • Universal fixative in Pathology is 10% neutral buffered formalin • For immunofluorescence testing -Michel’s transporting medium
Skin: Histology Epidermis and Dermis • Stratum Corneum • Stratum Granulosum • Stratum Spinosum • Stratum Basalis
1. DERMATITIS (eczema) • Non infective inflammatory reaction of the skin affecting the epidermis and dermis due to a variety of causes.
Dermatitis: Common Types & Pathogenesis • Allergic contact dermatitis - Type 1V hypersensitivity reaction • Irritant contact dermatitis - direct toxic effect, non immune • Nummular dermatitis -unknown cause • Atopic dermatitis - children- Type 1 (IgE mediated) hypersensitivity reaction
Dermatitis: Common Types & Pathogenesis • Seborrheic dermatitis - Pityrosporum ovale • Stasis dermatitis - venous stasis • Lichen Simplex Chronicus -repeated rubbing and scratching of skin
A question W chronic from acute dermatitis A) Lichenification B) Erythema and edema C) Vesicles and blisters D) Exudation E) Crusting
Dermatitis – 3 phases Pathophysiology 1) Acute dermatitis 2) Subacute dermatitis 3) Chronic dermatitis
Dermatitis – 3 phases Pathophysiology 1) Acute dermatitis - spongiosis, microvesicles (pain, erythema, edema, vesicles, itchy) 2) Subacute dermatitis - scaling, crusting 3) Chronic dermatitis - scaling and thickening of skin with increased skin markings (lichenification, related to repeated scratching) Important Integration slide
Acute Dermatitis Acute allergic contact dermatitis Poison Ivy
Acute dermatitis Acute atopic dermatitis
Subacute dermatitis Subacute atopic dermatitis
Chronic dermatitis Lichenification
Chronic dermatitis Lichenification
Acute D SPONGIOSIS: intercellular edema (A), microvesicles (B), dermal inflammation (C) A B C A Normal skin
Chronic D Lichenification: hyperkeratosis (A), acanthosis (B), dermal fibrosis (C) A B C Thickening of all layers of skin Normal skin
What single feature distinguishes chronic from acute dermatitis A) Lichenification B) Erythema and edema C) Vesicles and blisters D) Exudation E) Crusting Answer: A
2. PAPULOSQUAMOUS DISEASES • A group of etiologically unrelated skin disorders where lesions share a common clinical appearance -Papular, but may contain other forms, - well demarcated - scaly • Psoriasis, Lichen planus and Pityriasis rosea
Psoriasis: clinical forms • Psoriasis vulgaris - most common type • Guttate psoriasis • Pustular psoriasis • Erythrodermic psoriasis • Psoriatic nails • Psoriatic arthritis
Psoriasis Vulgaris vs Guttate Psoriasis Generalized, rapid onset, follow strep throat Discrete erythematous plaques, silvery white scale multiple smaller erythematous plaques, scale minimal
A Psoriasis Vulgaris case • Well circumscribed Erythematous (salmon pink) papules/plaques with silvery white scale • Kobner phenomenon: lesions appear at site of repeated trauma • Auspitz’s sign -removal of scale results in minute bleeding points
Auspitz sign Pinpoint bleeding areas where scale is removed
Psoriasis Vulgaris - Pathology Parakeratosis (silvery scale) Acanthosis Dilated vessels, dermal inflammation Inflammation and epidermal proliferation
Study Psoriasis -under the microscope A B C For information only
Psoriasis Pathophysiology • Increased epidermal turn over or shortened cell cycle from 311 to 36 hours which results in 28 times the normal production of epidermal cells of psoriatic skin • T cell mediated, CD4 T cells mediate epidermal proliferation • Stratum corneum is abnormally formed • Cause unclear, role for genetic and environmental factors
Pityriasis Rosea • Common, self limiting, disease of children • Cause is unknown, but may follow various infections, debate regarding HHV-7 (viral) • Herald patch -first lesion, larger • Symmetrial smaller lesions appear within 2 weeks on trunk, thighs and arms -christmas tree -like arrangement • Mostly a clinical diagnosis, biopsy rarely needed
Pityriasis Rosea Herald patch and multiple round or oval macules with fine scale at the periphery of each lesion CHRISTMAS TREE Herald patch
Lichen Planus (5 P’s) • Purple (violaceous) • Pruritic • Polygonal • Planar • Papules x Flat topped
Lichen Planus • Acute or chronic inflammatory dermatosis involving skin and mucous membrane • Idiopathic in most cases • Possible HLA associated genetic susceptibility
Lichen Planus Location Skin -flexural surfaces, wrists Mucous membrane-mouth Nail Hair loss Koebner phenomenon: lesions appear at site of trauma Hepatitis C has been associated
Lichen Planus -Pathology Hyperkeratosis (Scale) Irregular acanthosis Basal cell damage Band of lymphocytes Inflammatory injury to the basal cells of the epidermis leads to epidermal thickening and scaling
Study Lichen Planus: under the microscope A B C D For information only
Prepare • Vasculitis -common types, causes • Cutaneous manifestations of systemic disease - Diabetes - Lupus - Dermatomyositis • Drug reactions - common types • All signs and phenomenon • Acne