Download

1 / 44
650 likes | 3.49k Views
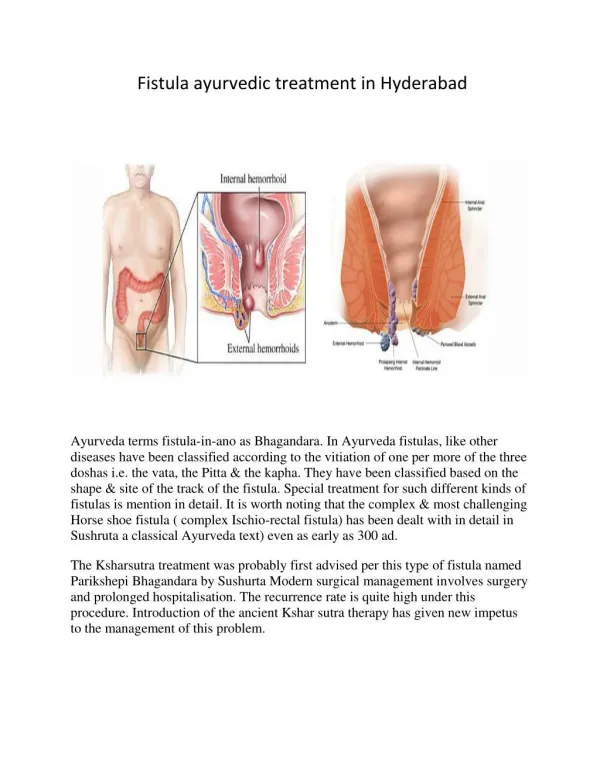
The Best Surgical Treatment for Fistula-in-ano. Dr John Wong PYNEH. Etiology. Cryptoglandular theory Trauma Foreign body Iatrogenic Malignancy Crohn’s disease Tuberculosis HIV. J.G.Williams et al. Colorectal Disease 2007. Classification. Park’s classification (1976).

E N D
The Best Surgical Treatment for Fistula-in-ano Dr John Wong PYNEH
Etiology • Cryptoglandular theory • Trauma • Foreign body • Iatrogenic • Malignancy • Crohn’s disease • Tuberculosis • HIV J.G.Williams et al. Colorectal Disease 2007
Classification • Park’s classification (1976) J.G.Williams et al. Colorectal Disease 2007
Goodsall’s rule 49% 90% J.G.Williams et al. Colorectal Disease 2007
Investigation • Indications: • Complex fistula • Impaired sphincter function • Suspicious of secondary cause
Investigation • Anatomy • Endoanal Ultrasound, MRI • Physiology • Anorectal manometry • Cause • Inflammatory marker, colonoscopy, rectal biopsy
Endoanal Ultrasound • High accuracy (93%) to identify the internal opening • Injection of hydrogen peroxide can increase the detection rate ANZ J. Surg. 2005; 75: 64-72 J.G.Williams et al. Colorectal Disease 2007
Endoanal Ultrasound • Disadvantage: • Pain and discomfort • Operator dependent • Limit field ~2cm from probe Limited use for trans-sphincteric or more complex FIA!
MRI • Gold standard • Multi-planar image • Show the fistula system in relation to the underlying anatomy • High sensitivity • Primary track: 86% • Secondary track: 91% • Horseshoe extesion 97% ANZ J. Surg. 2005; 75: 64-72 J.G.Williams et al. Colorectal Disease 2007
Principles of management • To drain abscess • To deal with the secondary track if any • Definitive treatment of the primary track Efficacy Continence
Fistulotomy • Lay-opening ofthe fistula track from external opening to internal opening • Inter-sphincteric fistula • Recurrence rate 0-21% • Disturbance in continence: 0 to 82% • Extent of external sphincter division: <30% J.G.Williams et al. Colorectal Disease 2007
Fistulectomy • Excision of the entire fistula track • Low lying fistula • No advantage in both recurrence and incontinence rate compared with fistulotomy • High lying fistula • ‘Core out’ technique + internal sphincterotomy Surgical intervention for anorectal fistula. The Cochrane Collaboration 2010
Seton Loose seton • Achieve drainage of the fistula track • Allow any secondary track to heal • As part of staged fistulotomy J.G.Williams et al. Colorectal Disease 2007
Staged fistulotomy • Low recurrence rate • Significant rate in incontinence • Major incontinence rate up to 42% J.G.Williams et al. Colorectal Disease 2007
Seton Tight (cutting) seton • Commonly used in high transphincteric fistula • Divide the muscle slowly to produce a gradual fistulotomy J.G.Williams et al. Colorectal Disease 2007
Low recurrence rate • Disturbance of fine control is common • Major incontinence rate >10% (up to 43%) J.G.Williams et al. Colorectal Disease 2007
Fibrin Glue • Fibrin clot to seal the track • Stimulate the migration, proliferation and activation of the fibroblasts • Sphincter-sparing method A.I. Malik & R.L. Nelson; Colorectal Disease 2008
Fibrin Glue • High recurrence rate • Long term healing rate(~14% - 60%) A.I. Malik & R.L. Nelson; Colorectal Disease 2008
Anal Fistula Plug • Sphincter-sparing method • Bioprosthetic plug • Internal opening must be identified
Anal Fistula Plug • Controversial results from different centre PYNEH 11 5 45% P. Garg et al. Colorectal Disease 2010 HYS Cheung et al. Surgical Practice 2009
Advancement Flap + core out fistulectomy • Sphincter-sparing method • Pre-op bowel prep and antibiotics cover • Internal opening must be identified
Advancement Flap + core out fistulectomy • Low long term success rate • High recurrence due to: • Small flap • Excessive tension J.G.Williams et al. Colorectal Disease 2007
LIFT • Ligation of Intersphincteric Fistula Tract • Rojanasakul in 2007
LIFT • Short term success rate was encouraging (~57-94%) • Long term result still unknown Arch Surg. 2011;146(9):1011-1016
Conclusion • No single best treatment for FIA • Treatment for FIA must be individualized • Types of the fistula • Premorbid sphincter function
Recommendation • Inter-sphincteric fistula (High / low lying, with or without internal opening) Fistulotomy
Recommendation • Extra-sphincteric fistula • Usually associated with an underlying cause • Treat the underlying cause • Drain any sepsis • Never disrupt or explore the sphincter
Exception for Goodsall’s rule • Horseshoe fistula • Long track that extend to the anterior quadrant of the anal canal • Crohn’s disease • Iatrogenic
Fistulogram • Accuracy ~16-50% only • Difficult to relate the track to the sphincter anatomy • The acute track are just column of granulation tissue without a lumen • Need external opening • Painful
Fistulotomy in acute anorectal sepsis • Pros: • decrease the rate of recurrent anorectal sepsis • Cons: • increase risk of impair continence • Some individuals would have unnecessary surgery • Fisulotomy should be performed when internal opening can be found and the fistula is submucosal or intersphincteric (low lying) J.G.Williams et al. Colorectal Disease 2007
Radiofrequency fistulotomy • Use of radio-wave as energy source • Less bleeding • Less pain • Quicker recovery • No difference in recurrence and incontinence rate Surgical intervention for anorectal fistula. The Cochrane Collaboration 2010
Fistulotomy with marsupialization • Suturing the edge of the track to its base • Less bleeding • Shorter healing time • No difference in recurrence and incontinence rate Surgical intervention for anorectal fistula. The Cochrane Collaboration 2010
Fistulotomy vs Fistulectomy • No difference in recurrence and incontinence rate A.I. Malik & R.L. Nelson; Colorectal Disease 2008
Chemical seton • Coated with layers of latex and plant extracts • Strong alkaline outer layer • Cut through tissue at a rate of 1cm every 6 days • More painful • Evidence on recurrence and healing rate remain inconclusive A.I. Malik & R.L. Nelson; Colorectal Disease 2008
Anal fistula plug • Better outcome in : • Deep trans-sphincteric fistula • Long track fistula • Narrow-gauge fistula
Advancement Flap • Contra-indications: • Presence of proctitis • Undrained sepsis • Malignant / radiation related fistula • Stricture of the anorectum • Severe sphincter defect • Severe peripheral scaring due to previous surgery J.G.Williams et al. Colorectal Disease 2007
FIA with Crohn’s disease • Medical treatment, eg. Anti TNF-alpha • Infliximab • Emergency treatment • Incision and drainage of the fistula • Stabilization • Insertion of seton to optimize drainage and medical therpay J.G.Williams et al. Colorectal Disease 2007
Incontinence scale • Flatus, mucus, liguid, solid stool • The Cleveland Clinic (Wexner) Incontinence Score • sum of 5 parameters is on a scale from 0 (=absent) to 4 (daily) frequency of incontinence to gas, liquid, solid, of need to wear pad, and of lifestyle changes.