Download
1 / 31
360 likes | 737 Views
Empiric Antibiotic Therapy. Antibiotics. The appropriate use of empiric antibiotics is central to medical practice. The goals of empiric antibiotic regimens are: To provide adequately broad coverage to treat an infection before the culprit organism is identified.

E N D
Antibiotics • The appropriate use of empiric antibiotics is central to medical practice. • The goals of empiric antibiotic regimens are: • To provide adequately broad coverage to treat an infection before the culprit organism is identified. • To use a sufficiently narrow spectrum of coverage so that antibiotic resistance and adverse drug reactions are minimized. • Review previous cultures and sensitivities • Always remember, the cornerstone of effective infectious treatment is good source control. -David Butler, MD, Infectious Disease UCSD
Antibiotics • Today we will discuss: • Specific regimens by organ system • Organisms to be worried about
Major infections in internal medicine • Pneumonia • Meningitis and encephalitis • Urinary tract infections • Cellulitis and other soft tissue infections • Fever in the neutropenic patient
“The captain of the men of death” • Pneumonia is the sixth-leading cause of death in the US • 4,000,000 cases/year in ambulatory patients • More than 600,000 admissions/year • ~14% mortality among inpatients • Likely higher in elderly inpatients
Common organisms • Streptococcus pneumoniae – most commonly identified cause of pneumonia across the board. • Haemophilus influenzae and parainfluenzae – second most common organisms in some studies; more common in smokers. • Mycoplasma pneumoniae and Chlamydophila pneumoniae– frequent pathogens among otherwise healthy people, often present atypically. • Legionella pneumophila – also considered an “atypical” organism, may be transmitted via fomites. • Moraxella, Streptococcus pyogenes (GAS).
Other organisms • Pseudomonas aeruginosa • Coccidioides immitis • Staphylococcus aureus • Klebsiella pneumoniae, E. coli, other GNRs • Mycobacterium tuberculosis • Pneumocystis jiroveci • Anaerobes: Bacteroides, Peptostreptococcus • Viruses
Pneumonia: Guidelines • ATS and IDSA guidelines for pneumonia recommend initial empiric therapy based on patient status and risk factors. • Patient categories based on clinical status, comorbidities, and risks for infection with: • penicillin- and multidrug-resistant pneumococci (MDRSP) • enteric Gram-negative organisms • Pseudomonas aeruginosa
Pneumonia: some random thoughts • Antibiotics within 4-8 hours • If someone is sick enough to be admitted, start with two drugs. • Use intravenous therapy up front. • Always get blood cultures beforehand. • Consider sputum cultures if feasible. • Remember the “red flags”: • Multilobar disease, effusions, upper lobe disease, mediastinal lymphadenopathy, cavitary lesions. • Again don’t write pneumonia and effusion in the same note without a tap procedure note soon to follow
Community-acquired pneumonia: regimens • Ceftriaxone and azithromycin • Ceftriaxone: 3rd generation cephalosporin (β-lactam) • Good coverage of S. pneumoniae, H. influenza, Moraxella. • Use higher doses in patients <50 years old: 2 g IV q24h. • Allergic reactions in PCN-allergic patients rare (3-5 %). • “Fun-fact” reaction: biliary sludging. • Azithromycin: macrolide • Covers the “atypicals”: Mycoplasma, Chlamydophila, Legionella • Reasonable pneumococcus coverage but resistance increasing. • Less GI upset than erythromycin. • Probably not suitable as outpatient monotherapy in San Diego.
Respiratory Fluoroquinolones • Moxifloxacin, Levofloxacin, and gatifloxacin (off the market). • Inhibitors of DNA gyrase. • Broad coverage of pneumococcus, Gram-negatives, atypicals. • Limited activity against Pseudomonas, Staphylococcus. • Ciprofloxacin has limited Gram-positive coverage but is better for Pseudomonas. • No anaerobic coverage.
Fluoroquinolones • Moxifloxacin and Levofloxacin are good monotherapy choices for CAP patients who can be treated as outpatients. • Moxifloxacin (Avelox) is the quinolone of choice at NMCSD • Do not have to dose based on renal function • DOES NOT cover UTI • Consider using with ceftriaxone for initial inpatient therapy. • Overuse is breeding resistance. • Adverse reactions of note: • QT prolongation (may be more of a concern with moxifloxacin). • Achilles tendon rupture (cipro) • Hypo/hyperglycemia, especially with gatifloxacin (which is why it’s off the market). • Relatively contraindicated in children.
Pneumonia: additional considerations • Consider aspiration risk in patients with alcohol/drug abuse, dementia, stroke. • Cover anaerobes with piperacillin/tazobactam. • Piperacillin/tazobactam (Zosyn™) • Anti-pseudomonal penicillin with β-lactamase inhibitor. • Broad coverage (Gram-positive, Gram-negative, anaerobes). • Moderate but less-than-fantastic staphylococcal coverage. • Indicated in hospital-acquired pneumonias: • Usual dose 3.375 g IV q6h, but 4.5 g IV q6h if concerned for Pseudomonas. • High sodium load (over 2 grams/day at usual doses). • Combine with moxifloxacin or levofloxacin for atypical coverage, ciprofloxacin or aminoglycosides for Pseudomonas.
Pneumonia: additional considerations • Why don’t patients get better? • Nosocomial infections with MSSA, MRSA (50% of all S. aureus) • Complicated pleural space • Fungal infections (esp. coccidioidomycosis) • Tuberculosis • Other infections • Consider PCP in the immunosuppressed or with HIV risk factors
Pneumonia summary • Community-acquired • Ceftriaxone 1-2 g IV q24h PLUS • Azithromycin 500 mg IV/PO q24h • Moxifloxacin 400 mg IV/PO q24h • Levofloxacin 750 mg IV/PO q24h • Hospital-acquired • Pip/Tazo 3.375-4.5 g IV q6h • +/- Vancomycin or Linezolid for MRSA coverage • Anaerobes • Pip/Tazo 3.375g IV q6h
Meningitis and encephalitis • CNS infections are common admitting diagnoses. • Common organisms: • Enteroviruses, HSV, maybe arboviruses? • Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae (rarer) • Mycobacteria, Coccidioides, Cryptococcus in special situations.
CSF evaluation • If possible, perform LP on side and get opening pressure especially if considering fungal or MTB • Cell count with differential – tube 1 and 4 • Protein, glucose • Gram stain and culture • Enterovirus and HSV PCR – ensure the ER sent it (makes you feel warm and fuzzy if you don’t think it’s bacterial) • Consider AFB and fungal cultures, cocci serology, crypto antigen if indicated. • Save extra CSF and hand-deliver samples to the lab. • For God’s sake, save extra CSF and hand-deliver samples to the lab.
Empiric treatment of meningitis • Generally healthy adults: • Ceftriaxone 2 g IV q12h • Vancomycin 15 mg/kg IV q12h, could talk to pharmacy about q8 hour dosing if young healthy patient (Troughs 15-20) • For coverage of MDRSP until cultures available or negative. • Probably does not cause renal impairment alone. • Consider dexamethasone 0.15mg/kg IV q6h with first dose for confirmed or highly-suspected bacterial meningitis continue for 48-96 hours. • If patients are elderly, immunosuppressed, pregnant, or alcoholic, add ampicillin 2 g IV q4h for coverage of Listeria monocytogenes. • If encephalitis is a concern, add HSV coverage with acyclovir 10 mg/kg IV q8h. • Remember to maintain adequate urine output (15cc/kg/day).
Extra thoughts on meningitis • In patients with more insidious presentations and markedly elevated CSF protein, consider: • Coccidioidal meningitis • Lymphocytic pleocytosis in the CSF with elevated protein. • Initial treatment with at least fluconazole 800 mg PO q24h – lifelong therapy indicated if diagnosis confirmed. • Cryptococcal meningitis • Always high on the differential in HIV. • India ink stain good for quick diagnosis although CSF antigen is probably a better test. • Treated with ampho B and flucytosine initially. • Tuberculous meningitis • Especially in subacute patients with appropriate travel/exposure history. • Probably should be talking with ID if you’ve reached this point.
Neurological infections summary • Start with ceftriaxone 2 g IV q12h and vancomycin 15 mg/kg IV q12h. • Add ampicillin 2 g IV q4h if immunosuppressed, >50 years, or alcoholic. • Acyclovir 10 mg/kg IV q8h if encephalitic. • Fluconazole 800 mg PO q24h (at least) if cocci is a major concern. • Remember LFT monitoring when using azoles.
Pyelonephritis • Clinically presents with CVA tenderness, fever, and pyuria in most patients. • May be more subtle in the elderly and immunosuppressed. • Urinalysis and culture are mandatory and should be obtained prior to antibiotics in the hospitalized patient. • Common organisms: • Escherichia coli • Other GNRs: Proteus, Enterobacter, Klebsiella, Providencia • Enterococcus faecalis and faecium
Urine Gram stain • For some mysterious reason, urine is the one body fluid not routinely stained by the lab. • Call 2-9234 and ask for a Gram stain. • Gram-negative rods • E. coli, other Enterobacteriaciae. • Start with a quinolone (cipro, levo) – moxi not effective. • Alternatives: ceftriaxone 1-2 g IV q24h, gentamicin 5 mg/kg IV q24h. • Gram-positive cocci • Group B strep, Enterococcus, Staphylococcus saprophyticus. • Treat with ampicillin 2 g IV q4h once confirmed -> might start with vancomycin empirically. • Consider vancomycin in patients with Foleys or recent hospitaliztion. • Note that E. faecium=VRE (approx 10%) -> rare at NMCSD. • S. aureus in the urine = bacteremia/endocarditis until proven otherwise.
Complicated UTIs • Persistent fever on appropriate antibiotics for 72 hours: obtain renal ultrasound to rule out perinephric abscess. • Renal obstruction, renal transplant, indwelling catheters: • Consider additional coverage for Pseudomonas, Enterobacter, Acinetobacter. • Pip/tazo may be appropriate for broader coverage • Candiduria may be treated with short courses of oral fluconazole. • I don’t generally advocate treating candiduria in an asymptomatic patient, but treatment may be warranted if the patient is febrile or otherwise symptomatic with pyuria on UA. • E. faecium may represent VRE – this would be treated with linezolid 600 mg PO/IV q12h, but don’t treat all enterococci empirically as though they’re VRE. • Nausea, diarrhea, and thrombocytopenia are all common side effects of linezolid.
Pyelonephritis summary • E. coli and other GNRs are most common and respond well to quinolones in general. • Suspect Enterococcus if GPCs are found on Gram stain. • Vancomycin 15 mg/kg IV q12h or ampicillin 2 g IV q4h (if sensitive). • Consider vancomycin in the recently hospitalized • E. faecium may be VRE – would treat with linezolid or daptomycin in most cases. • Consider Pip/tazo in complicated UTIs. • Pip/tazo will cover E. faecalis (if sensitive). • 14 days of total therapy is generally recommended, especially in β-lactam-based regimens.
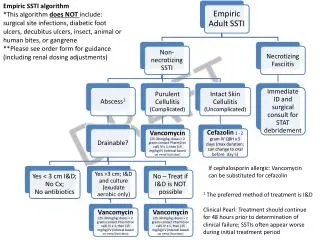
Cellulitis and soft-tissue infections • Staphylococcus aureus and Streptococcus pyogenes (group A β hemolytic streptococci - GABHS). • GABHS tends to evolve more rapidly and may have regional lymphadenopathy and lymphatic streaking on exam. • Admissions usually for failure of outpatient treatment. • Think MRSA, especially in patients from MCRD and NSWC. • Initial regimens: • Vancomycin 15 mg/kg g IV q12h • If MSSA or streptococci are confirmed: • Nafcillin or oxacillin 2 g IV q4h • Cefazolin 1 g IV q8h • Clindamycin 900 mg IV q8h
Special considerations • Necrotizing fasciitis • Consider when pain is intense or rapidly progressive. • Early surgical consultation and debridement. • Antibiotics are only an adjunct to surgery: • Clindamycin 900 mg IV q8h AND • Unasyn 3 g IV q6h OR Pip/Tazo 3.375 g IV q6h AND • Vancomycin 15 mg/kg IV q12h (dose for troughs 15-20). • Diabetic foot infections • Generally polymicrobial (GPCs, GNRs, anaerobes). • Empiric coverage: • Pip/Tazo 3.375 g IV q6h • Clindamycin 900 mg IV q8h and ciprofloxacin 400 mg IV q12h • Concider Augmentin as outpt therapy with close follow-up • Duration of therapy depends on tissue viability and the presence/absence of osteomyelitis.
Fever in neutropenia • Temperature ≥38.3C x 1 or ≥38.0C for > 1 hour • Absolute neutrophil count <500 (or <1000 and expected to be less than 500 in the next 24 hours) • Total WBCs x (% PMNs + % bands) • Numerous causes, specific etiology may not be isolated. • Pneumonia: pneumococcus, Klebsiella, E. coli, Pseudomonas. • Urinary tract: E. coli, Proteus, Klebsiella, Enterococcus • Mucositis: S. viridans • Indwelling catheters: S. aureus, coagulase-negative staphylococci, Candida. • Viruses, invasive fungal pathogens, non-infectious sources of fever.
Initial empiric management • Thorough history and physical exam, including oral cavity, indwelling lines, perirectal region. • Blood and urine cultures, chest radiograph, sputum if available. • Separate cultures from catheter sites. • Fungal isolators. • Initial antibiotics: • Pip/Tazo 4.5 g IV q6h and tobramycin 5mg/kg IV q24 • Cefepime 2 g IV q8h • Aztreonam 2 g IV q6-8h and vancomycin 1-1.5 g IV q12h if PCN-allergic. • Add vancomycin to patients if suspicious of Gram-positive UTIs, catheter infections, mucositis, or prior MRSA infections. • Other regimens (e.g., Pip/Tazo alone, meropenem alone) appear effective; institutions will vary in their “routine” regimen. • Don’t forget aggressive fluid resuscitation in the septic patient.
Additional notes • Consider adding metronidazole 500 mg IV q6h if highly suspicious of an anaerobic infection OR if C. difficile is a concern (oral metronidazole preferable for C. difficile). • Empiric antivirals generally not indicated, but acyclovir 10 mg/kg IV q8h appropriate if vesicular or ulcerated lesions are noted on exam. • If no improvement after 3-5 days of broad-spectrum antibiotics, add antifungals. • Traditional drug of choice: amphotericin B • Today, typically we use caspofungin or voriconazole. • Removal of indwelling catheters mandatory if patient is septic or if S. aureus is isolated from the blood. • Consider echocardiography if bacteremic with a new murmur.
Final comments • Get cultures before antibiotics whenever possible. • Review CHCS frequently for results or check out the lab personally. • Remember to adjust dosing for renal insufficiency. • MDRD algorithm – www.nephron.com • Check Sanford for dosage adjustments. • Be familiar with common adverse reactions. • If you’re thinking about using the exotic drugs, you might want to think about consulting ID. • Be aware of the FORBIDDEN LIST OF ANTIBIOTICS THAT REQUIRE I.D. APPROVAL. • Meropenem, Imipenem, Ertapenem, Linezolid, Daptomycin, Synercid, Colistin, Tigecycline