Download

1 / 14
150 likes | 304 Views
Achieving glycaemic targets with basal insulin in T2DM by individualizing treatment. Fonseca, V. A. & Haggar, M. A. Nat. Rev. Endocrinol. 10, 276–281 (2014). Introduction. Type 2 diabetes mellitus (T2DM) is a major clinical problem in practice

E N D
Achieving glycaemic targets with basal insulin in T2DM by individualizing treatment Fonseca, V. A. & Haggar, M. A. Nat. Rev. Endocrinol. 10, 276–281 (2014)
Introduction • Type 2 diabetes mellitus (T2DM) is a major clinical problem in practice • The natural history of T2DM actually starts well before the diagnosis, with obesity and insulin resistance • Insulin secretion is vital for the physiological maintenance of glucose regulation • Insulin is essential for glucose clearance from the circulation into skeletal muscle or adipose tissue, and for suppressing hepatic glucose production both in fasting state & after ingestion of a meal
Introduction • The purpose of this Review is to highlight the importance of insulin in the treatment of T2DM and, more importantly, to focus on the addition of basal insulin to oral agents to provide treatment that is individualized to achieve glycaemic targets • This Review will also identify major considerations regarding insulin treatment in different types of patients with T2DM, and how to overcome barriers to insulin therapy
Individualizing targets and therapy • Over the past decade, several major clinical trials have examined the role of intensive glycaemic control on complications of DM • Importantly, the ACCORD, ADVANCE and VADT trials failed to demonstrate a reduction in cardiovascular-related adverse events with intensive glycaemic control • It is important to recognize that in these trials patients were selected very late in the natural history of the disease when most of them had already developed diabetic complications
Individualizing targets and therapy • Following the publication of these trials, the goal of glycaemic control in patients with T2DM has been the subject of intense debate • HbA1c targets are now recommended to be individualized, particularly for patients who have a long history of T2DM, multiple comorbidities and limited life expectancy • On the other hand, low HbA1c targets (that is, <6.5%) can be appropriate for individuals who have short duration of the disease, long life expectancy and no clinically significant comorbidities, particularly cardiovascular disease
Where does insulin ‘fit’ in therapy? • No general rule exists to dictate the time of initiation of insulin therapy • However, guidelines of the American Association of Clinical Endocrinologists and the Canadian Diabetes Association suggest considering insulin treatment at the time of T2DM diagnosis if glycaemic control is very poor (HbA1c levels >9%) & the patient is symptomatic • The American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) guidelines for the management of hyperglycaemia in T2DM recommend that initial insulin therapy be considered for patients who present for the first time with T2DM and an HbA1c level >10%
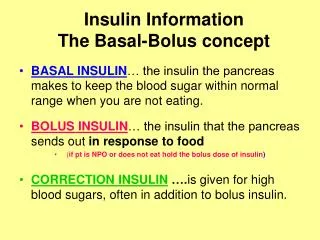
Replacing insulin physiologically • The primary goal of insulin replacement is to mimic a normal physiological insulin response, which consists of basal insulin between meals and a boost of insulin at mealtimes • It is given either in the form of a bolus injection or a bolus with an insulin pump at mealtimes • Other than with pumps, such physiological replacement can only be achieved by using basal insulin with prandial insulin at mealtimes • However, in patients who are taking oral agents, it may be possible for a few years to manage glycaemic control with basal insulin alone
Replacing insulin physiologically • On the basis of various trials, the ADA/EASD algorithm recommends the addition of basal insulin only to an oral agent and continuation of therapy with the oral agent • If this fails, a second type of insulin could be tried, either in the form of a premixed insulin injected twice daily or continuing therapy with basal insulin & adding a rapid-acting injection with the main meal • Following failure of that regimen, it may be necessary for patients to take three or more injections and more complex regimens involving basal insulin plus multiple mealtime rapid-acting insulin agents
Which basal insulin should be chosen? • Several comparative trials have been carried out for different types of insulin. The overall conclusion is that any insulin will lower the glucose and HbA1c level substantially, but all are associated with some weight gain and some increased risk of hypoglycaemia • The larger the doses and the more aggressive the titration, the lower the HbA1c level achieved but also the greater the possibility of adverse effects, such as hypoglycaemia • Therefore, a more appropriate goal may be HbA1c level lowering that does not increase the risk of hypoglycaemia considerably, instead of HbA1c level lowering alone
Barriers to insulin therapy & suggested solutions • Feelings of failure of self-care: Educate patients about type 2 diabetes mellitus and the natural progression of the disease process • Fear of disease: Identify concerns through careful patient assessment. Use a patient-centred approach and include the patient when setting goals • Complexity of treatment: Minimize the number of injections per day. Use pens instead of syringes • Embarrassment associated with self-injection in public: Highlight the convenience and discreteness of new injecting devices such as covered safety needles and pens
Barriers to insulin therapy & suggested solutions • Fear of needles: Use desensitization techniques and/or insulin pens • Financial concerns: Inform patients that there are several generic insulin medications. Remind patients that assistance programmes are often available • Weight gain: Educate patients on diet and exercise • Hypoglycaemia: Begin the diabetic education process early. Teach patients how to perform self-monitoring of blood glucose levels and how to recognize and manage hypoglycaemia
The appropriate patient for insulin • All patients with T2DM should be considered as potential candidates for intensive insulin therapy; however, there are certain considerations regarding insulin therapy for different types of patients • In pregnant women, insulin is the traditional first-choice drug to achieve optimal glycaemic control • The first trimester is often the period when the risk of hypoglycaemic events associated with the use of insulin is the highest, and insulin therapy should be especially closely monitored and adjusted during this period
The appropriate patient for insulin • Since insulin dosing is based on body weight, children’s insulin requirements change frequently as they undergo growth spurts & puberty • Children often need assistance with diabetes self-care skills, such as rotating injection sites, and require a good support system, which can include neighbours and/or teachers • Ederly patients with T2DM often require special attention, such as assessing their capacity for self-injection and continually reassessing their status and circumstances • In patients with CKD, doses need to be titrated carefully, and patients receiving insulin who develop renal disease can require a dose reduction
Conclusion • In many patients with T2DM, as β‑cell dysfunction progresses, treatment with oral agents fails to maintain adequate glycaemic control • Clinical inertia and futile strategies can lead to suboptimal metabolic outcomes & increase the risk of disease-related complications • Insulin should be added whenever it is needed to achieve glycaemic control • Therapy should be individualized on the basis of personalized HbA1c goals and the patient’s ability to engage in self-management • Although all types of insulin are effective, ultimately the choice of insulin type depends on the preferences of the patient and clinician