Download
1 / 68
700 likes | 1.01k Views
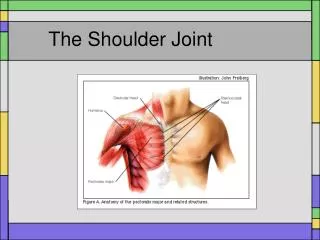
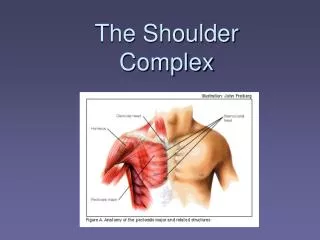
The Shoulder. Claire Bailey & Elizabeth Bowman Bsc (Hons) Physiotherapy April 2013 Email: mail@roundwoodclinic.co.uk. Aims. Diagnostic categories Evidence based decision making? Treatment options When to refer on (or not?!). Anterior GHJ Anatomy. The Rotator Cuff. Introduction.

E N D
The Shoulder Claire Bailey & Elizabeth Bowman Bsc (Hons) Physiotherapy April 2013 Email: mail@roundwoodclinic.co.uk
Aims • Diagnostic categories • Evidence based decision making? • Treatment options • When to refer on (or not?!)
Introduction • Shoulder pain third most common MSK complaint • 15% referred for physiotherapy in the 3 years following their initial consultations • Peak incidence 4-6th decades • 50% acute GHJ pain resolves in 8-10 weeks • Linsell et al (2006)
Red Flags • History of Ca, mass, swelling etc. • Red skin, fever, systemically unwell ?infection • Trauma, epileptic fit, loss of rotation • Unexplained significant sensory or motor deficit • Visceral referred pain
Frozen Shoulder “it comes on slowly; (with) pain usually felt near the insertion of the deltoid; inability to sleep on the affected side; painful and incomplete elevation and external rotation; restriction of both spasmodic and mildly adherent type; atrophy of the spinati; little local tenderness; (&) x-rays negative except for bone atrophy”. Codman (1934)
Frozen shoulder cont. • Elusive underlying pathology • ?inflammatory ?scarring ?enzyme • Pain predominant or stiffness predominant (Hanchard et al. 2011) • Primary (unknown cause) • Secondary (to trauma) • 2% population; 935 patients; 58% female • Dominant side 52%; bilateral 38% (Chambler et al. BMJ 2003)
Secondary frozen shoulder • Trauma • R.Cuff tear • Post –operatively • Diabetes • Cerebral haemorrhage • Thyroid • Autoimmune disease • Cervical spine pathology • Hormonal changes • Prolonged immobilisation • Algodystrophic
Stages of frozen shoulder Freezing Pain increases with movement and is often worse at night. There is a progressive loss of ROM with increasing pain. Lasts approx. 2-9/12 Frozen Pain begins to diminish, ROM much more limited (50%). Lasts approx. 4-12/12 Thawing Condition may begin to resolve. Most patients experience a gradual restoration of motion over next 12-42/12
Clinical Picture • Insidious onset • Pain at deltoid insertion • Night pain • Pain at rest • Reduced AROM and PROM • Reduced ER (restriction >50% of the opposite side) • Normal x-rays
Frozen shoulder x-rays • NORMAL • To exclude:- • Cuff arthropathy/massive cuff tear with secondary OA changes • OA – bony end feel, osteophytes limit ER • Dislocation locked – stuck in IR causing avascular necrosis to humeral head ALL LIMIT ER, THEREFORE, TENTATIVE DIAGNOSIS WITHOUT X-RAY
Treatment • Neglect? (better in 2 years) • Physiotherapy • Injection – improved shoulder related disability @ 6/52 (Ryans et al. 2005) • MUA / arthroscopic release – significant loss of ER not changing with rehabilitation @ 6-9 months
Conservative management • Explanation • Modify activities • Analgesia • Physiotherapy? • Corticosteroid injection? • CONSIDER EARLY REFERRAL IF....... • Patients pain is particularly disabling to them • Severe restriction in PROM inhibiting function • Considering operative or specialist management
Surgical management • Symptoms and function are unchanging and significantly disabling after 6/12 of conservative treatment • Arthroscopic release +/- SAD • ? MUA • ?hydrodilation • Suprascapular nerve block – improves pain but not movement
Impingement • Up to 74% patients presenting in primary care SAIS • Physiotherapy first line Rx • Roy et al. (2008) • Ostar (2005)
Classification • Primary (intrinsic) • Secondary (extrinsic) • Outlet / non-outlet • External / internal impingement • Bursal side wear and tear not substantiated by histological studies – majority on articular side
Impingement cont. • Extrinsic theory challenged • Irritation causes tendonitis and bursitis? • “sub-acromial pain syndrome” pain related to the bursa rather than the mechanical impingement effect. (Lewis 2011) • Reactive tendonopathy to tendon disrepair and subsequent degeneration. • Dysfunction of the r.cuff = bursitis and Sx
Impingement • Rotator cuff strain • Tears • Calcific tendonitis • Tendonopathy due to chronic overuse • Indirect causes - GHJ instability • SLAP • Abnormal muscle patterning
Clinical Presentation • Difficulty with over head activities • Pain mid range arc • Constant background ache / night pain / increased pain on movement = ? Inflammation in bursa (only place to find inflammation in impingement)
Diagnosis • Impingement tests • Neers • Hawkins • Weakness in ER • X-ray AP, axillary – spur formation, sclerosis, acromion type (>3/12 symptoms) • U/S to confirm and exclude cuff tear
Impingement Treatment • Physiotherapy • NSAID’s? If constant pain • ?Injection – short term efficacy only and most effective at 1-2/52 when constant pain (Trojian 2005) • ?Poor outcome with surgery following repeated injections • Conservative treatment minimum 8/52 • Surgery SAD
Rotator Cuff tears • Almost all tears are chronic and degenerative in nature • Often insidious history • Can occur after trauma or dislocations • Similar Sx to impingement • ? Clinically obvious weakness
Diagnosis • Drop arm test • Severe pain, profound weakness of abduction, or an inability to maintain the arm in 90O abduction then slowly lower • Positive infraspinatus testing (ER) • Pain that awakens the patient at night (Riddle 2001). • Tests may be better at ruling out cuff tears rather then detecting them • ultrasound
Acute rotator cuff tear • Patients presenting with a traumatic history, sudden or progressive weakness • Urgent U/S and referral • Consider early repair • 6-12/52 window of opportunity for best outcome from surgery
Chronic symptomatic cuff tear • ?non-operative management for 3-6/12 • Advice / NSAID’s?/ physiotherapy • X1 steroid injection? • Failed non-operative management re-evaluation consider U/S or MRI • Only need surgery if warranted by Sx • ?SAD for pain relief and to avoid the long rehab. required for cuff repairs if the patient has – good movement, strength
Full thickness cuff tears – non-operative management • “tincture of time” • Physiotherapy • NSAID’s??? • Modified activities • Steroid injection?? • ? Can compensate due to activation of residual intact cuff • Partial tear vs. Impingement ?does it matter as doesn't change outcome/type of Rx
AC Joint Dysfunction • Traumatic v degenerative onset • Traumatic onset is usually a fall on to the point of the shoulder and can involve • Stretching or tearing of the acromioclavicular or coracoacromial ligaments • Subluxation/dislocation of the AC joint • Degenerative problems tend to occur in individuals over 45 years
Clinical Presentation • Degenerative • Pain with activity and ?at rest over ACJ (may radiate in to traps region but not deltoid) • ?ROM restricted in to overhead elevation • No obvious inflammatory signs • Traumatic • Reports a traumatic onset • May be an observable deformity • May also be associated with sub-acromial impingement
Diagnosis • Pain on palpation over ACJ • Pain on active adduction (Scarf test) • Pain on O’Brien’s • X-ray may be used to exclude osteolysis/oes-acromially or to define degree of disruption in traumatic onset
Treatment • Rockwood classification for traumatic disruption • Type I & II managed conservatively • Type III individual cases • Type IV – IV managed surgically • Physiotherapy • ?injection therapy • Surgical options in degenerative cases if failed conservative management
Glenohumeral Instability • Instability is the abnormal motion of the glenohumeral joint that may include subluxation or dislocation, co-existing laxity, pain • Involves one or more (usually a combination) of ligaments, tendons, glenoid labrum, joint capsule • Traumatic instability v atraumatic instability