Download
1 / 46
480 likes | 741 Views
Acute and Chronic Liver Disease. Dr. Orla Crosbie Consultant Gastroenterologist, CUH 4 th Med, 17 th Nov 2010. Contents. Investigations Acute Liver disease Chronic Liver Disease. Normal Liver Function. Protein synthesis and degradation: albumin, transport proteins, clotting factors,

E N D
Acute and Chronic Liver Disease Dr. Orla Crosbie Consultant Gastroenterologist, CUH 4th Med, 17th Nov 2010
Contents • Investigations • Acute Liver disease • Chronic Liver Disease
Normal Liver Function • Protein synthesis and degradation: • albumin, transport proteins, clotting factors, • Carbohydrate metabolism • Lipid metabolism • Bile acid metabolism • Bilirubin metabolism • Hormone inactivation • Drug inactivation and excretion • Immunological function
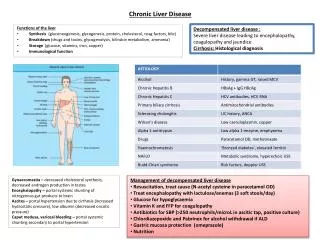
Liver function tests 1 • Bilirubin – Conjugated and Unconjugated • ALT/AST levels • Alkaline Phosphatase • gGT • Albumin • INR • FBC
Liver function tests 2 • Hepatitis antibodies: A, B, C….D, E • EBV, Toxo, CMV, Leptospirosis • Ferritin and fasting transferrin saturation, • Haemochromatosis genetics • Caeruloplasmin and copper (serum), • 24 hour urine for copper • Autoantibodies: ANA, ASMA, AMA, Coeliac • Immunoglobulins: IgG, IgA, IgM • Cholesterol, triglycerides, glucose, TFTs • a1antitrypsin levels + phenotype • a-fetoprotein (cirrhotics only)
Imaging • Ultrasound – Liver substance, lesions, gallbladder and biliary tree, vessels (Doppler exam), spleen size and varices • CT scan – confirm small lesions, see pancreas • MRI of Liver – classify smaller lesions • MRCP: Magnetic resonance cholangiopancreatography, to see the biliary tree • ERCP: Endoscopic retrograde cholangiopancreatography– diagnostic and therapeutic: stones, strictures etc.
Liver Biopsy • Very useful for confirming a diagnosis, staging degree of inflammation and/or fibrosis, iron content, mass lesions • Contraindications: Bleeding disorders, ascites, small liver, uncooperative patient • Complications: Bleeding, pain, perforation another viscus, biliary leak, pneumothorax • Methods: Percutaneous, transjugular, laparoscopically
Jaundice • Pre hepatic • Haemolysis • Conjugation abnormalities • Hepatic – any liver disease, acute or chronic • Post hepatic – Obstruction
Gilberts syndrome • Deficient glucuronyl transferase • Unconjugated hyperbilirubinaemia, other LFTs normal • 2-5% population • Jaundice when dehydrated • Low grade haemolysis • Normal liver, life expectancy etc.
Acute Liver Disease • Infections • Viral Hepatitis A, B, C, D, E, EBV, CMV, HSV, • Others – Leptospirosis, Toxoplasma, • Drugs – MANY – HERBALS/OTC • Alcohol • Poisons • Vascular obstruction (eg. Budd Chiari)
Acute Liver Disease • SYMPTOMS Nausea & vomiting, diarrhoea, cholestasis, pyrexia, abdominal pain, jaundice Fulminant/acute liver failure rare, patient very unwell coagulopathy and encephalopathic • SIGNS Jaundice, hepatomegaly, abdominal tenderness + splenomegaly, flap/foetar
Acute Liver Disease: treatment • Supportive mainly • Remove precipitating cause if known eg. drugs • Treat some cases eg. Leptospirosis, some viral infections in acute phase, • Expect complications and treat as they arise eg: • Infection • Bleeding • Outcome • Resolve • Worsen and develop FLF (? Transplant) • Progress to chronic liver disease, may require specific therapy*
Paracetamol toxicity • Present in many preparations*** • 10gms (20 tablets) can cause fatal liver failure • Initial N&V often settles with symptoms of liver failure developing 2-3 days later • Coagulopathy and raised ALT • Paracetamol levels may be low/neg by this stage • High index of suspicion • Treat if in any doubt with N-acetylcysteine
Chronic Liver Disease • Alcohol • Autoimmune – autoimmmune hepatitis, PBC (Primary Biliary cirrhosis), PSC (Primary Sclerosing Cholangitis) • Haemochromatosis • Chronic Viral hepatitis: B & C • Non-alcoholic fatty liver disease (NAFLD) • Drugs (MTX, amiodarone) • Cystic fibrosis, a1antitryptin deficiency, Wilsons disease, • Vascular problems (Portal hypertension + liver disease) • Cryptogenic • Others: sarcoidosis, amyloid, schistosomiasis
Chronic Liver Disease - symptoms • None • Fatigue • Malnutrition • Ascites, ankle oedema, pleural effusions – weight gain • Impotence • Bleeding • Jaundice, itch, steatorrhoea
Alcohol • Fatty liver – may have no symptoms • Alcoholic Hepatitis – can be unwell with liver and renal failure, jaundice, coagulopathy • Cirrhosisand its complications • Can present at any stage above • ACCURATE ALCOHOL HISTORY • Clues: LFTS: gGT, MCV • Other problems: medical (pancreatitis, malnutrition, infections, cardiac), social….
Tx. Of Alcoholic Hepatitis • Feed (Enterally) • Vitamin replacement: Thiamine: IV Pabrinex and multivitamins • Treat DTs • Corticosteroids if Maddrey’s discriminant function higher than 32: • 50% mortality rate • mDF= 4.6 x (PT patient-control) + Bilirubin/17.1 umol/L • Treat with steroids: Prednisolone 40mg X1/12 • Other scoring systems: Glasgow Alcoholic Hepatitis Score, MELD score
Fatty Liver • Many Secondary causes of fatty liver, including drugs, alcohol, previous surgery • Primary fatty liver or non-alcoholic fatty liver disease (NAFLD) commonly recognised now • Some patients in addition to fat on liver biopsy can have inflammation as well (steatohepatitis) and are referred to as NASH (non- alcoholic steatohepatitis), a portion of these will develop scarring and can progress to cirrhosis over time • Is associated with obesity, non-insulin dependent diabetes, dyslipidaemia and hypertension; considered part of syndrome X/metabolic syndrome • Fatty liver getting more common – obesity increasing.
Hereditary haemochromatosis • Commonest genetic problem N. European • Progressive iron overload leading to liver disease (cirrhosis and hepatocellular carcinoma), diabetes, pigmentation, arthropathy, hypogonadism, cardiac…. • Not always symptomatic at diagnosis
Hereditary haemochromatosis • Need high serum ferritin level and fasting transferrin saturations to make diagnosis • Fasting Transferrin Saturation > 45% • Raised Serum Ferritin > 350ug/L • Genetics: C282Y and H63D mutation • REMEMBER: MANY CAUSES OF RAISED FERRITIN
Hereditary haemochromatosis • If HH confirmed • LFTs and ultrasound +/- Liver biopsy to diagnose Cirrhosis • Prognosis worse if diabetic or cirrhotic at time of diagnosis • If cirrhotic, need tumour surveillance • Treatment is phlebotomy to render iron deficient and prevent organ damage, does not remove risk of HCC • Life long
Chronic Liver Disease - Decompensation • Ascites + renal failure • GI bleeding • Encephalopathy • Jaundice • Hepatocellular carcinoma
Ascites • Associated with a poor prognosis • Often associated with ankle oedema, pleural effusions • Diagnostic paracentesis: 1. Biochemistry, 2. Micro & 3. Cytology • SAAG: Serum albumin/ascites gradient > 11g/dl • Risk of Spontaneous Bacterial Peritonitis • Therapy • Low salt diet • Diuretics: Spironolactone and Frusemide • Therapeutic large volume paracentesis – albumin replacement • Shunts – TIPS • Transplantation • DAILY WEIGHTS, WATCH U&Es • Don’t fluid restrict
Spontaneous Bacterial Peritonitis • Risk: Ascites and Chronic liver disease • Often vague symptoms • Diagnosis: Diagnostic paracentesis for • WCC > 250 cells/mm3 and mainly polymorphs • Culture • Usually Gram negatives • Treat antibiotics +/- albumin • Antibiotic prophylaxis
Variceal bleeding • Due to portal hypertension • Varices at porto-systemic anastomoses • Skin – Caput medusa • Oesophageal & Gastric • Rectal • Posterior abdominal wall • Stomal • Medical emergency
Resuscitate patient Good IV access Cross-match blood and clotting factors Emergency OGD
Band oesophageal varices Can Inject gastric varices with glue Manage in HDU/ITU Terlipressin IV Prophylactic antibiotics U/sound and doppler portal vein Rebleed: Rescope, Balloon tamponade, May need TIPPs shunt, transplant
Prevention of variceal haemorrhage • PRIMARY PREVENTION: Have not bled • Scope all cirrhotics • If large varices: B block with Propranolol or Band varices. • SECONDARY PREVENTION: After bleed • Repeat banding until varices eradicated +/- propranolol (ideally measure portal pressures)
Encephalopathy • Confusion due to liver disease • Graded 1-4 • Precipitants: GI bleed, infection, constipation, dehydration, medication esp. sedation • Flap – asterixis and hepatic foetar • Treat underlying cause, • Laxatives – phosphate enemas and lactulose • Rifaximin-broad non absorbed spectrum antibiotic
Hepatorenal syndrome • Progressive renal failure in the setting of advanced liver disease and portal hypertension • Rule out other causes for renal failure: Pre-renal, Microscopy, ultrasound • Type 1 (acute) and Type 2 (chronic) • Very poor prognosis
Hepatocellular Carcinoma (Hepatoma) • Primary Liver Cancer • Usually in setting of cirrhosis • Risk factors: Viral hepatitis B/C, Alcohol, haemochromatosis, a1 anti-trypsin, male PBCs • Screen cirrhotics with 6 monthly u/sound and afetoprotein levels • Diagnosis made on imaging (u/s, CT or MRI) and aFP levels in cirrhotics – biopsy usually not done • Cure: transplant or surgery • Palliation: TACE, radiofrequency ablation, Sorafenib po.
Liver transplantation • INDICATIONS: • Fulminant Liver failure determined by certain clinical criteria (King’s criteria) • Paracetamol Overdose: pH, INR, creatinine and Encephalopathy • Non-paracetamol: INR, Bilirubin, age, cause, encephalopathy • Chronic Liver Disease: Mainly for Decompensation • ascites • Uncontrolled variceal haemorrhage • Encephalopathy • Hepatoma – Milan criteria • Disease specific criteria: Rising Bilirubin in PBC • Need to consider Q of Life and Other illnesses
Liver transplantation • WAITING LIST: MELD scoring system • Liver Matched by blood group and size • Post operative • Immunosuppression to prevent rejection eg. Tacrolimus, Mycophenolate and Steroids • Prophylaxis against infection eg. CMV, HSV, PCP • Can get graft failure, vascular thrombosis, rejection (acute and chronic), infections, disease recurrence…
Liver disease: summary • LFTs • Causes of jaundice • Causes of acute hepatitis • Causes of cirrhosis – Risk factors • Symptoms and Signs of liver disease – Ascites, encephalopathy & SBP, variceal haemorrhage, HCC and hepatorenal syndrome.