Download
1 / 1
10 likes | 173 Views
Metrics for a Mastoidectomy Simulator. Stanford University Departments of Computer Science and Surgery. Funding provided in part by the Stanford Bio-X Program and the National Institutes of Health.

E N D
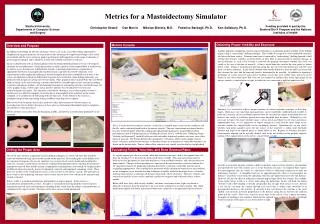
Metrics for a Mastoidectomy Simulator Stanford University Departments of Computer Science and Surgery Funding provided in part by the Stanford Bio-X Program and the National Institutes of Health Christopher Sewell Dan Morris Nikolas Blevins, M.D. Federico Barbagli, Ph.D. Ken Salisbury, Ph.D. Obtaining Proper Visibility and Exposure Modern Minimally Invasive Surgery (MIS) Metrics Console Overview and Purpose Another important component of good surgical technique is maintaining proper visibility of the drilling region, using a “saucerizing” drilling technique. This enables the surgeon to avoid vulnerable structures just below the bone surface. If instead some bone is removed by “undercutting” (drilling beneath a shelf of bone that obscures visibility, as shown below at left), there is increased risk of structure damage. In our environment, as each voxel of bone is removed, the program determines whether this voxel was visible to the user at the time of removal. A line is traced from the voxel to the view point, as shown below center. Points at small discrete intervals along this line are tested for intersection with the voxel mesh (via direct indexing). If any voxels (beyond some threshold distance from the drill) are intersected, they obstruct the view and the removed voxel is determined to be invisible. In addition to reporting a percentage of voxels removed with correct visibility, voxels that were visible when removed can be shown in one color while those that were not are rendered in another color in the right panel of our metrics console, as shown below at right, in which the user saucerized at right but undercut at left. Miniaturization In addition to providing the obvious advantages of low-cost, easily-accessible training opportunities, computerized surgical simulators are in position to take advantage of complete knowledge of the virtual environment and the user’s actions to analyze performance with regards to a wide range of elements of good surgical technique and to afford the trainee with valuable constructive criticism. In close collaboration with an otolaryngologist from the Stanford Medical School, we have developed a simulator for mastoidectomy, a surgical procedure in which a portion of the temporal bone is drilled away in order to access the inner ear. A hybrid data structure is maintained that allows computation of appropriate drill forces using rapid collision-detection in a spatially-discretized volumetric voxel representation while graphically rendering a smooth triangular mesh that is modified in real-time as the voxels are drilled away. Realistic drill sounds, based on data recorded in a bone drilling laboratory, are produced, with frequencies giving cues to bone depth. Other graphical effects include bone dust and blood (both of which can be removed using a suction controlled by a second haptic device) rendered according to particle simulations, shadows, detailed anatomical models of surrounding structures and of the inner ear, stereo graphics using a Cyberscope, and an intuitive interface for switching between tools and maneuvering the view point. The simulator is networked, allowing a user at onecomputer to observe another user on a different computer, to feel the forces being applied in the simulator on the remote computer, or to collaboratively drill along with the other user. At the bottom of the screen is a neurophysiology monitor, providing realistic feedback regarding nerve response. Most of our work on metrics thus far has made use of this infrastructure to evaluate trainees in mastoidectomy, but we believe that many of these ideas are fundamental throughout surgery and plan to extend them to other procedures. Below are three screen shots from the beginning, middle, and end of a mastoidectomy performed on our simulator. Similarly, it is essential to achieve proper exposure of critical anatomic structures so that their shapes, which may vary somewhat among patients, can be confidently established and avoided. A point on a structure can be considered exposed when the ray from the camera to the point does not intersect any voxels at a distance greater than some threshold from the point. Although it is not necessary to expose the entire structure, many, such as nerves and blood vessels, twist and turn in unpredictable ways, so it is imperative to expose enough of it such that the entire shape of the structure (within the surgical field) can be confidently inferred. Quantitatively, we can check whether each point (sampled across the top surface of the structure) is within some threshold distance and angle of an exposed point, as shown below at left. Regions of structures that have been properly exposed can be specially shaded, such as the red shading on the properly exposed portion of the sigmoid shown in the metrics console below at right. This is a screen shot of our metrics console. A data file is recorded when a user runs the simulator, and this file can be read and played back in the metrics console. The user’s movements are played back in real time in the left panel, while the continuously updated right panel gives visual feedback about performance (such as drilling region [see “Drilling the Proper Area”], visibility [see “Obtaining Proper Visibility and Exposure”], and drill collisions with vulnerable structures) against a cut-away view of the inner ear anatomy. The bottom left provides quantitative evaluations, while various graphs (such as forces, velocities, and bone removal rates as functions of time or of distances to vulnerable structures) are shown on the bottom right. Various sliders allow extensive user control over the displays and playback. Evaluating Forces, Velocities, and Bone Removal Rates Drilling the Proper Area As a good surgeon gets closer to certain vulnerable anatomic structures, such as the sigmoid sinus, the dura, the facial nerve, or the inner ear, he/she drills more carefully. This increased caution may be reflected in such parameters as decreased drill forces, decreased drill velocities, and a decreased rate of bone removal. Changes in these quantities as a function of distance from these structures indicate that the surgeon recognizes the landmarks indicating that he/she is nearing a vulnerable structure and is responding appropriately. By recording these parameters while experienced surgeons use our simulator, we are attempting to use machine learning techniques to build a model of the proper forces, velocities, and bone removal rates as functions of distances from each of these structures. The force, velocity, and removal rate profiles of users of the simulator can then be compared and evaluated relative to these models. Below, drill force (left), drill velocity (middle), and bone voxel removal rate (right) are shown as functions of distance from the facial nerve for a run of the simulator by an expert surgeon. The expert drilled more lightly and slowly and removed bone more cautiously as he approached the facial nerve. One of the more obvious components of good drilling technique is to remove all bone that should be removed without removing any bone that should not be removed. By recording the voxels drilled away by experienced surgeons who use our simulator, we can learn which voxels should and should not be removed. A trainee’s performance can then be evaluated both quantitatively, by reporting the amount of improperly removed bone and the amount of improperly remaining bone, and visually, by displaying dots of different colors for properly removed, improperly removed, and improperly remaining voxels. These three sets of dots can be visualized all at once, or one at a time in our metrics console. The proximity of these voxels to key underlying structures can be seen in our cut-away view, which can be translated and rotated as desired. Below, at left, is a model mastoidectomy performed by an expert surgeon. In the center is a mastoidectomy performed by a novice. At right is a visualization showing properly removed (green), improperly removed (red), and improperly remaining (blue) voxels from the trainee’s mastoidectomy, as compared to the expert’s model. Structures of the inner ear are visible underneath. In order to accurately measure a trainee’s ability to properly expose critical structures, the simulator must provide the user with realistic cues as to the structures’ locations. In temporal bone surgery, the most important cues are visual, as a thin layer of bone is sufficiently translucent to make out underlying structures. A straightforward way of approximating this effect is to precompute the distances of all bone voxels from the underlying structures and shade them inversely with distance. However, this has the effect of making the structure appear larger all the way around. For example, in the figure below at left, if a viewer looks along the dotted line, he/she will think the brown structure (with yellow shading) is directly along his/her line of sight, when in fact it is not. Instead, a ray can be cast from the camera through each voxel that is within some threshold of its precomputed distance to the structure. If and only if this ray intersects the structure is the voxel shaded, with intensity inversely proportional to the distance along the ray between the collision point and the voxel. These rays must be recast only at the end of every camera movement. Examples of shading in our simulator, bluish for the sigmoid sinus, redish for the dura, and bright white for regions of the inner ear, are shown below at right.