Download
1 / 70
710 likes | 930 Views
LECTURE DEGENERATIVE DISEASES OF THE JOINTS AND SPINE COLUMN (OSTEOARTHRITIS, OSTEOCHONDROSIS). Definition. Also known as degenerative joint disease or “wear and tear arthritis”. Progressive loss of cartilage with remodeling of subchondral bone and progressive deformity of the joint (s).

E N D
LECTURE DEGENERATIVE DISEASES OF THE JOINTS AND SPINE COLUMN (OSTEOARTHRITIS, OSTEOCHONDROSIS).
Definition • Also known as degenerative joint disease or “wear and tear arthritis”. • Progressive loss of cartilage with remodeling of subchondral bone and progressive deformity of the joint (s). • Cartilage destruction may be a result of a variety of etiologies
Osteoarthritis (OA) - Definition • The repair mechanisms of tissue absorption and synthesis get out of balance and result in osteophyte formation (bone spurs) and bone cysts A case of the, “Which came first? The chicken or the egg?”
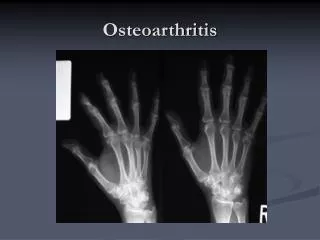
Osteoarthritis (OA) • OA is the most common form of arthritis and the most common joint disease • Most of the people who have OA are older than age 45, and women are more commonly affected than men. • OA most often occurs at the ends of the fingers, thumbs, neck, lower back, knees, and hips.
OA – Risk Factors Age • Age is the strongest risk factor for OA. Although OA can start in young adulthood, if you are over 45 years old, you are at higher risk. Female gender • In general, arthritis occurs more frequently in women than in men. Before age 45, OA occurs more frequently in men; after age 45, OA is more common in women. OA of the hand is particularly common among women. Joint alignment • People with joints that move or fit together incorrectly, such as bow legs, a dislocated hip, or double-jointedness, are more likely to develop OA in those joints.
OA – Risk Factors Hereditary gene defect • A defect in one of thegenes responsible for the cartilage component collagen can cause deterioration of cartilage. Joint injury or overuse caused by physical labor or sports • Traumatic injury (ex. Ligament or meniscal tears) to the knee or hip increases your risk for developing OA in these joints. Joints that are used repeatedly in certain jobs may be more likely to develop OA because of injury or overuse. Obesity • Being overweight during midlife or the later years is among the strongest risk factors for OA of the knee.
OA – Symptoms • OA usually occurs slowly - It may be many years before the damage to the joint becomes noticeable • Only a third of people whose X-rays show OA report pain or other symptoms: • Steady or intermittent pain in a joint • Stiffness that tends to follow periods of inactivity, such as sleep or sitting • Swelling or tenderness in one or more joints [not necessarily occurring on both sides of the body at the same time] • Crunching feeling or sound of bone rubbing on bone (called crepitus) when the joint is used
OA – Radiographic Diagnosis Asymmetrical joint space narrowing from loss of articular cartilage The medial (inside) part of the knee is most commonly affected by osteoarthritis.
left: Normal x-ray • Right: worn away cartilage reflected by decreased joint space
OA – Radiographic Diagnosis • Asymmetrical joint space narrowing • Periarticular sclerosis • Osteophytes • Sub-chrondral bone cysts
Joint space narrowing where there is more stress • Subchondral bone has thickened • bony overgrowth
significant joint space narrowing as well as proliferative bone formation around the femoral neck (arrows)
Left: normal hip Right: There is some joint space medially but the superior portion is completely destroyed. Supralateral aspects affected most because the weight is transfered through the roof of the acetabulum. Note the sclerosis and oseophyte formation (arrow).
painful bone on bone contact at the CMC joint and the large bone spurs -- osteophytes.
What to look for in an x-ray • Radiographic changes visible relatively late in the disease • Subchondral sclerosis • Joint space narrowing esp where there is stress • Subchondral cysts • Osteophytes • Bone mineralization should be normal
X-ray shows lateral osteophytes, varus deformity, narrow joint space in a 70 yr old female with OA
Clinical features and diagnosis • Pain Sources • Joint effusion and stretching of the joint capsule • Torn menisci • Inflammation of periarticular bursae • Periarticular muscle spasm • Psychological factors • Deep, aching localized to the joint • Slow in onset • Worsened with activity in initial stages • Occurs at rest with advanced disease
May be referred eg hip pain referred to the thigh, groin, knee. • Pain may be aggravated with weather changes
Exam • Joint line tenderness • Bony enlargement of joint • +/- effusion • Crepitus • Decreased range of motion
Joint exam • Joint line pain can indicate tear of the lining of the capsule or the meniscus. • Where is the patella?
Joint exam • In the evaluation of joint line pain, perform a varus or valgus stress test. • Apply stress across the joint, place fingers directly over the joint line to assess for pain, a clunk may indicate a meniscal tear, or crepitus may indicate cartilage damage.
Have the patient to lie supine on the exam table with leg muscles relaxed • Press the patella downward and quickly release it. • the patella visibly rebounds. • What does this mean? • a large knee effusion • Ballotable patella
Have the patient lie supine with leg muscles relaxed • Compress the suprapatellar pouch with your thumb, palm, and index finger. • "Milk" downward and laterally so that any excess fluid collects on the medial side. • Tap gently over the collected fluid and observe the effect on the lateral side • A fullness on the lateral side indicates the presence small knee effusion
Involved joints • DIP, PIP • 1st carpometacarpal • cervical/lumbar facet joints • 1st metatarsophalangeal • Hips • Knees • Uncommon • Wrist, elbows, shoulders, ankles
1st metatarso-phalangeal most commonly affected in OA of the foot.
OA – Arthroscopic Diagnosis Normal Articular Cartilage Ostearthritic degenerated cartilage with exposed subchondral bone Arthroscopy allows earlier diagnosis by demonstrating the more subtle cartilage changes that are not visible on x-ray
OA – Disease Management • OA is a condition which progresses slowly over a period of many years and cannot be cured • Treatment is directed at decreasing the symptoms of the condition, and slowing the progress of the condition • Functional treatment goals: • Limit pain • Increase range of motion • Increase muscle strength
Treatment • Non-pharmacokinetic • No proven medication-based disease modifying intervention exists. • Analgesics (acetominophen) • NSAIDS Help pain symptoms but controversial for long term use in non-inflammatory OA because of risks vs benefits • Narcotics • Intra-articular steroids • Chondroprotective agents • Anti-depressants
Intra-articular corticosteroids • May be used if NSAIDS are contraindicated, persistent pain despite use of other medications. • (not > 4 injections per year per joint) • 2004 meta-analysis of controlled trials (w/ placebo) showed short term improvement in knee pain, but efficacy in other joints is uncertain. • saline vs steroid injection? • A study comparing the two in knee OA showed no effect on joint space narrowing or significant difference in pain at the end of the study, but over a 2 yr period saline injections has less pain relief.
Intra-articular hyaluronans • Evidence shows they have a small advantage in terms of pain control, compared to intra-articular placebos or NSAIDS. • No evidence for improvement in function • Two studies comparing intra-articular steroids to hyaluronans have come to opposite conclusions-more trials are needed.
Intra-articular Corticosteroids • Beneficial in KNEE • LOE 1a • Beneficial in HIP • LOE 1b • Short-duration benefits: 2-4 weeks • Every 3 mos OK; not effective at 2 years
Intra-Articular Hyaluronic Acid (IAHA)“viscosupplement” • Very effective in knee and hip • LOE 1a for knee pain, fxn, & stiffness • Effective in ankle, shoulder (LOE lower) • Delayed effect (4 weeks) • Long duration (6 months) • 1-5 weekly injections
IAHA: Mechanism of Action • Increased synovial fluid HA conc. • Increased cartilage lubrication/elasticity • Chondrocyte proliferation • Chondrocyte stimulation matrix • Decreased inflammatory mediators • Inhibition of nociceptors • MAY BE DISEASE-MODIFYING • HIGH-M.W. prep’s have higher effects in vitro Devine, Shaffer. Use of viscosupplementation for knee osteoarthritis: an update. Curr Sports Med Rep 2011
OA – Non-operative Treatments • Pain medications • Physical therapy • Walking aids • Shock absorption • Re-alignment through orthotics • Limit strain to affected areas
Summary and Review • Low-impact exercise and strength exercise effectively treat OA • Minimize use of chronic NSAIDs • Viscosupplement injections give long-lasting pain reduction • Consider use of multiple treatments simultaneously • Arthroscopic lavage & debridement no better than conservative mgmt
Surgery • Arthroscopy • Cartilage transplantation • Joint replacement
Proximal Tibial Osteotomy • Osteoarthritis usually affects the inside half (medial compartment) of the knee more often than the outside (lateral compartment). • This can lead to the lower extremity becoming slightly bowlegged, or in medical terms, a genu varum deformity
Proximal Tibial Osteotomy • The result is that the weight bearing line of the lower extremity moves more medially (towards the medial compartment of the knee). • The end result is that there is more pressure on the medial joint surfaces, which leads to more pain and faster degeneration. • In some cases, re-aligning the angles in the lower extremity can result in shifting the weight-bearing line to the lateral compartment of the knee. This, presumably, places the majority of the weight-bearing force into a healthier compartment. The result is to reduce the pain and delay the progression of the degeneration of the medial compartment.
Proximal Tibial Osteotomy • In the procedure to realign the angles, a wedge of bone is removed from the lateral side of the upper tibia. • A staple or plate and screws are used to hold the bone in place until it heals. • This converts the extremity from being bow-legged to knock-kneed. • The Proximal Tibial Osteotomy buys some time before ultimately needing to perform a total knee replacement. The operation probably lasts for 5-7 years if successful.
Osteotomy Realignment of Joints Transfer Weight to less involved part of joint 60s and 70s Less popular Does not provide good long term results
Total Knee Replacement • The ultimate solution for osteoarthritis of the knee is to replace the joint surfaces with an artificial knee joint: • Usually only considered in people over the age of 60 • Artificial knee joints last about 12 years in an elderly population • Not recommended in younger patients because: • The younger the patient, the more likely the artificial joint will fail • Replacing the knee the second and third time is much harder and much less likely to succeed. • Younger patients are more active and place more stress on the artificial joint, that can lead to loosening and failure earlier • Younger patients are also more likely to outlive their artificial joint, and will almost surely require a revision at some point down the road. • Younger patients sometimes require the surgery (simply because no other acceptable solution is available to treat their condition)
Total Knee Replacement • The ends of the femur, tibia, and patella are shaped to accept the artificial surfaces. • The end result is that all moving surfaces of the knee are metal against plastic