Download
1 / 68
680 likes | 951 Views
Neuropsychiatric Manifestations of HIV. Thomas Newton, MD UCLA/Pacific AIDS Education and Training Center tnewton@mednet.ucla.edu. AIDS Education & Training Centers’ National Resources. Warmline: (800) 933 - 3413 PEPline: (888) 448 – 4911 (888) HIV - 4911

E N D
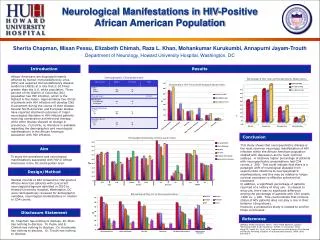
Neuropsychiatric Manifestations of HIV Thomas Newton, MD UCLA/Pacific AIDS Education and Training Center tnewton@mednet.ucla.edu
AIDS Education & Training Centers’ National Resources Warmline: (800) 933 - 3413 PEPline: (888) 448 – 4911 (888) HIV - 4911 Perinatal Hotline: (888) 448 - 8765 www.aids-etc.org
Neuropsychiatric Manifestations of HIV: Educational Objectives At the end of presentation, participants will be able to: • Identify risk factors for impairment • Discuss treatment options • Identify potential drug interactions
Neuropsychiatric Manifestations of HIV • Biologic • Psychologic • Social
KEY POINTS • HIV has global impact • Effects can be understood on variety of dimensions • Biologic effects related to host/virus interaction • Psychologic effects related to neuropsychiatric impacts and pre-existing vulnerabilities • Social effects vary by time and place
Biologic • Complications depend on severity of immunosuppression • Differential diagnosis changes • Early, middle and late stages of illness
Earlydefinition: • Above 400-500 CD4+, asymptomatic • Non HIV-related psychiatric syndromes more likely • Be wary of off, early presentations of HIV-related syndromes
KEY POINTS • High CD4 usually found early in infection, but… • Rate of progression extremely variable Case of Multidrug-Resistant HIV andRapid Progression to AIDS in New York City Background
On February 11th 2005, New York City health officials reported that a local gay man in his mid-40s had recently been infected with multidrug-resistant HIV and progressed rapidly to AIDS. He also has a history of unprotected sex while using methamphetamine. The man was first diagnosed with HIV between four and twenty months before steep drop in CD4 cells and a high viral load.
Middledefinition: • Roughly between 200 and 500 CD4+ • Mild symptoms • Before AIDS-defining O.I. (symptoms more important)
KEY POINTS • Lower CD4 levels generally found later in the disease, but… HIV-1 Evolution and Chemokine Receptor Genotypes-Implication for AIDS Progression
Genetic polymorphysms of chemokine receptor genes (CCR5, CCR2, CXCR4) are closely associated with AIDS. These chemokine receptors are coreceptors with CD4 for HIV-1, mutations in which confer protection against HIV-1 infection and/or slow progression of the disease.
The absence of CCR5 in ~1% of Caucasians very strongly protects against HIV-1 transmission. It is estimated that 25-30% of patients who remain AIDS-free for >16 years attribute their survival to mutations in these receptors. The protective mutation (delta32-CCR5) is not present in Africans or Asians who bear the burden of most of the world's HIV infection.
Latedefinition: • Below 200 CD4+ • After AIDS-defining O.I. • Very late: below 50 CD4+ (symptoms predict symptoms)
KEY POINTS • What about patients who once had CD4 < 200, but now … • …have CD4 > 500 • …continue with CD4 < 200, but virally suppressed?
Neuropsychiatric complications • Minimal early course of illness • Develop after other symptoms, usually • By death, probably more than 50% prevalence (really unknown)
KEY POINTS • …Early in illness, psychological symptoms are psychological until proven otherwise • …Late in illness, psychological symptoms are due to HIV until proven otherwise
KEY POINTS • …Difficult to determine if any symptom is due to HIV or other process • …Diagnosis and treatment guided by risk factors and probabilities
Neuropsyiatric complicationscont. • “Personality change” frequent, with increased lability • Memory, praxis, “cortical” abilities spared • A subcortical dementia, more like Parkinson’s than Alzheimer’s • Infrequent psychosis or mania (poorly defined)
KEY POINTS • What about patients who once had CD4 < 200, but now … …have CD4 > 500 …continue with CD4 < 200, but virally suppressed
Patient with CD4 > 500, but continued cognitive impairment Patient with CD4 < 200, but normal with methylphenidate (dependent on methamphetamine 15 years ago, now low risk for relapse)
Clinical Manifestations of HIV-related dementia Cognitive impairments --Short-term memory deficit; “forgetfulness” rather than amnesia --Decreased concentration and attention --Confusion and disorientation --Overall intellectual ability generally well preserved until late Visuospatial perception deficits Changes in personality or behavior --Apathy, decreased interest --Impaired judgment, erratic behavior --Social withdrawal --Rigidity of thought --Speech impairment: slow, dysarthria, hyphonia; difficulty in following other speakers
KEY POINTS • …Mini Mental State not helpful; detects delirium or “cortical” impairments • …Best screen is history + assessment of psychomotor speed
Early Entry • Confirmed by intrathecal antibody synthesis • Virus often retrieved from CSF • Probably ubiquitous
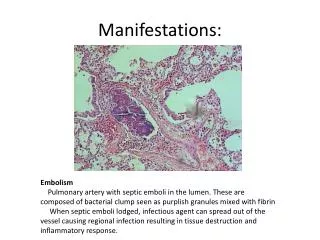
Indirect pathogenesis • Infection of non-neuronal cells important • Infection activates CNS macrophages • Activated macrophages produce toxic products • Viral products may be neurotoxic
KEY POINTS • …Other viruses infect neurons • …Herpes, rabies • …These produce irreversible deficits • …HIV produces combination of reversible and irreversible deficits
HIV and Brain Fig. 1. Cortical thinning on the lateral brain surface in HIV/AIDS. (a) Average profile of cortical thickness in AIDS patients. Right hemisphere is on the left. (b) Mean cortical thickness for matched healthy controls. (c) Average percentage thinning of the cortex in AIDS relative to healthy controls. (d) Color-coded map that shows the significance of the group difference, at each cortical point (reds indicate significant cortical thinning). The band of thinner cortex encompasses the primary sensorimotor, premotor, and parietal cortices. Thompson PM, Dutton RA, Hayashi KM, et al (2005): Thinning of the cerebral cortex visualized in HIV/AIDS reflects CD4+ T lymphocyte decline. PNAS 102:15647-52.
KEY POINTS • …Affects mood as well as cognition • …Unknown if pre-existing mood disorder risk factor • …Unknown roll of alcohol, cocaine, methamphetamine
Neuropsychiatric manifestations of HIVdimensions: • Biologic • Psychologic • Social
Depressiondiagnosis: • Differential diagnosis of “DUO” • Adjustment response • “Organic”---secondary to HIV-related disease • Medication complication (antiretroviral) • Psychiatric disorder
Psychologicbackground: • Illness occurs in context of numerous losses • Friends and loved may also be ill
Psychologicdepression: • May be more common in gay men regardless of HIV • Lifetime prevalence* in gay man of Major depression: 33% vs 3% Substance abuse: 45% vs 15% (ECA estimates for straight men) * Williams et al. Arch Gen. Psychiatry, 1991
Depressiondiagnosis: Important considerations: • Onset and course • Symptoms and severity • Previous episodes and treatment response (remember, treatment is easy, diagnosis is hard)
DepressionAfter correct diagnosis: • Controlled trials suggest standard antidepressants have usual efficacy • Anecdotal evidence for “replacement” therapies (testosterone) • Psychotherapy helpful for dealing with loss, etc. • Stimulants useful in advanced illness
Psychologicanxiety: • Situational anxiety expected, responds to benzodiazepines • Sleep disturbance expected, responds to standard treatment • Cognitive/behavioral treatments helpful when anxiety is reality based
Stressful Life Events and HIV • Coping in Health and Illness Project (CHIP at UNC) • 9 year longitudinal study • Life events and difficulties • Interviewer based • Severity, duration, and context important • Excludes events due to HIV Leserman et al., CNS Spectrums 8:25-30 2003
CHIPS • At baseline, severe life events in previous 6 months: • Low NK cells (CD16+ and CD56+) • Fewer CD8+
CHIPS • For each severe stressor: • Risk of AIDS-defining condition tripled • For those above median in stress: • AIDS progression rate was 74%, • compared to 40% for those below median in stress Leserman et al., Psychol Med 32:1059-1073 (2002)
KEY POINTS • Stressor depends on individual • Best assessed using personal impact, duration of impact, and change needed to accommodate • Lists of stressors (Holmes and Rahe) fair but can be missleading
CHIPS • Limitations: • Small sample (99) • Geographically limited (N.C.) • Lack of control for duration of HIV infection • Completed prior to HAART
CHIPS • Convergence of • AIDS diagnosis • HIV stage progression • Cellular indices of progression • Suggest validity
KEY POINTS Unknown: • Would treatment alter impact of stressor? • Who’s at greatest risk? • What factors are protective?
UCLA Study • Bereavement associated with more rapid decline in CD4 cells • Not accounted for by differences in health habits, drug use, age • Finding meaning in bereavement mitigated against decline Bower et al., J Consult Clin Psychol 66:979-986 (1998)
KEY POINTS • “Stress” can be toxic or beneficial • Mechanism unknown • What aspects of immune function impacted not always clear
Pharmacokinetic Mechanisms of Drug Interactions • Altered drug absorption • Inhibition of metabolism • Induction of metabolism
SystemicCirculation OralMedication HepaticArtery HepaticVein Intestine PortalVein -P450 -P450 Enzymes present in intestinal cells Directly metabolized here before reaching systemic circulation -PGP First Pass Metabolism
Pharmacodynamic Mechanisms of Drug Interactions • Synergism • Antagonism • D4T and AZT • IDV and SQV • Can effect drug activity or toxicity • Ritonavir + saquinavir in liver enzymes or cholesterol • AZT + ganciclovir enhanced bone marrow suppression • d4T + ddI worsened neuropathy