Download
1 / 208
2.12k likes | 2.38k Views
Anemias. Definition. Reduction of total RBC MASS below average levels Reduction of oxygen carrying capacity of the blood Leads to tissue hypoxia

E N D
Definition • Reduction of total RBC MASS below average levels • Reduction of oxygen carrying capacity of the blood • Leads to tissue hypoxia • Practically, measure by Hemoglobin concentration, and Hematocrit (ratio of packed RBCs to total blood volume). They correlate well with anemia when the plasma volume is normal
Classification of anemia according to cause • Blood loss: acute, chronic • Diminished RBC production • Increased destruction (hemolytic anemia) • Extrinsic factors (infection, antibody, mechanical) • Intrinsic RBC abnormalities: 1) Hereditary (membrane, enzyme, Hg abnormalities) 2) Acquired (Paroxysmal nocturnal hematuria)
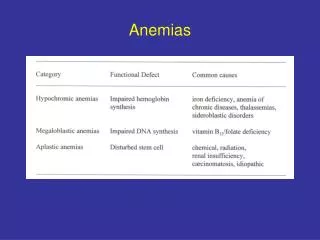
Classification of anemia • According to morphology: • Size: normo, micro, macrocytic • Color: normo, hypochromic • Shape: anisopoikelocytosis (spherocytes, sickle, schistiocytes) • Hypochromicmicrocytic anemia usually reflects impaired Hg synthesis • Macrocytic anemia reflects stem cell disease and maturation
RBC indices • Hg concentration, Men: 13.8-18.0 g/dL, Women: 12-15 • Hematocrit: volume % of RBCs in blood, 45% men, 40% women • Mean Cell Volume (MCV): average size in femtoliter, 10−15 (normal: 80-99 fL) • Mean Cell Hg (MCH): average mass of Hg inside the RBC in picograms, 10−12, normal (27-31) • Mean Cell Hg Concentration (MCHC): the average concentration of Hg in a given volume of packed red cells, expressed in grams per deciliter • RBC count: number of cells/L Male: 4.7-6.1 million/ microliter Female: 4.2-5.4 • Reticulocyte index (0.5-1.5%) • Red cell distribution width (RDW): the coefficient of variation in red cell volume
Clinical features of anemia • Dizziness • Fatigue • Pallor • Headache • Hypotension • Tachycardia • Dyspnea • Special types: jaundice, bone and joint pain, growth retardation
Anemia of acute blood loss • Symptoms are related to decreased intravascular volume, might cause cardiovascular shock and death • Body responds by shifting fluid from interstitial to intravascular space, causing dilutional anemia and hypoxia • Erythropoietin secretion is stimulated, activating BM erythropoiesis • Mature RBCs as well as Reticulocytes appear in blood after 5 days • In internal hemorrhage, iron is restored from extravasated RBCs and used again in erythropoiesis • In external and GIT hemorrhage, iron is lost, which complicated anemia • The anemia is normochromicnormocytic, with reticulocytosis • Leukocytosis (secondary to stress) • Thrombocytosis (secondary to high erythropoietin)
Anemia of chronic blood loss • Occurs when the rate of RBC loss exceeds regeneration • Mostly associated with iron deficiency anemia
Hemolytic Anemia • Normally, RBCs age is around 120 days, aged RBCs are engulfed by phagocytic cells in spleen, liver and BM • In Hemolytic anemia; premature destruction of RBCs • Accumulation of Hg degradation products • Secondary increased erythropoiesis • Extravascularhemolysis: increased phagocytic activity • Intravascular hemolysis: occurs inside blood vessels
ExtravascularHemolysis • Generally caused when the RBC is less deformable or having abnormal shape • Abnormal RBC shape prevents its normal movement in splenic sinusoids • Prolonged time of RBCs passage attracts histiocytesto engulf them • Free Hg from destructed RBCs binds Haptoglobin in serum • Hg within phagocytes is converted to bilirubin • The triad of extravascular HA is: Anemia, splenomegaly and jaundice
Intravascular Hemolysis • Less common • Caused by mechanical damage, complement fixation, microorganism, exogenous toxins • Due to large amount of free Hg, haptoglobin is cleared from the serum • free Hg in serum is oxidized to Methemoglobin (metHg), • Excess free Hg and met Hg are excreted in urine (hemoglobinuria) causing dark urine • Renal hemosiderosis may occur
Hereditary Spherocytosis • This inherited disorder is caused by intrinsic defects in the red cell membrane skeleton that render red cells spheroid, less deformable, and vulnerable to splenic sequestration and destruction • The prevalence of HS is highest in northern Europe • AD inheritance pattern, in 75% of cases • The remaining patients have a more severe form of the disease that is usually caused by the inheritance of two different defects (a state known as compound heterozygosity)
Pathophysiology • Normal RBC is durable and elastic • Spectrin is the major internal membrane protein, consists of two helical polypeptides; α, β • The tail of Spectrin binds Actin • Spectrin-Actin complex, is connected by Ankyrin and band 4.2 to band 3, a transmembrane protein • Protein 4.1 binds the tail of spectrin to Glycophorin A, a transmembrane protein
Pathophysiology • Various mutations involving α-spectrin, β-spectrin, ankyrin, band 4.2, or band 3 that weaken the interactions between these proteins cause red cells to lose membrane fragments • Most mutations are frame-shift, resulting in absent protein • To accommodate the resultant change in the ratio of surface area to volume these cells adopt an irreversible spherical shape • Spherocytic cells are less deformable than normal ones and therefore become trapped in the splenic cords, where they are phagocytosed by macrophages • Na+influx in spherocytes is twice than normal, while K+efflux is the same, facilitating hemolysis in the microenvironment of the spleen • RBC Life span is dropped to less than 20 days
Clinical features • Congestion of RBCs in the spleen causes splenomegaly and anemia • Jaundice, pigmented gall bladder stones • Reticulocytosis, BM erythroid hyperplasia, hemosiderosis • Family Hx of anemia or splenectomy • Abnormal osmotic fragility test • Increased MCHC in 50% of cases • Treatment: splenectomy
Morphology • Blood film: RBCs are round, small, hyperchromatic, no visible central pallor • “Howell-Jolly” bodies are seen in post splenectomy. A fragment of chromosome which is detached and left in the cytoplasm after the extrusion of the nucleus, secondary to accelerated erythropoiesis. Appears as 1 or 2 eccentric dots
Spherocytes appear as small, round cells without the central pallor. Howell Jolly bodies are noted
Glucose-6-Phosphate Dehydrogenase Deficiency • G6PD reduces nicotinamide adenine dinucleotide phosphate (NADP) to NADPH while oxidizing glucose-6-phosphate • NADPH then provides reducing equivalents needed which protects against oxidant injury by catalyzing the breakdown of compounds such as H2O2 • G6PD deficiency is a recessive X-linked trait, placing males at higher risk for symptomatic disease.
Types of G6PD deficiency • Several hundred G6PD genetic variants are known, but most are harmless • The normal enzyme is G6PD-B • Only two variants, designated G6PD-A and G6PD Mediterranean, cause most of the clinically significant hemolytic anemias • G6PD-A is present in about 10% of American blacks; G6PD Mediterranean is prevalent in the Middle East
Pathophysiology • The half-life of G6PD-A is moderately reduced, whereas that of G6PD Mediterranean is functionally abnormal • Because mature red cells do not synthesize new proteins, G6PD-A or G6PD Mediterranean enzyme activities fall quickly to levels inadequate to protect against oxidant stress as red cells age. Thus, older red cells are much more prone to hemolysis than younger ones
Pathophysiology • Oxidants cause both intravascular and extravascularhemolysis in G6PD-deficient individuals • Exposure of G6PD-deficient red cells to high levels of oxidants causes the cross-linking of reactive sulfhydryl groups on globin chains, which become denatured and form membrane-bound precipitates known as Heinz bodies • These are seen as dark inclusions within red cells stained with crystal violet. Heinz bodies can damage the membrane sufficiently to cause intravascular hemolysis • Splenic macrophages identify Heinz bodies and pluck them out resulting in indentation. The remaining RBC is known as “bite cells”
Causes of hemolytic crisis • Hemolysis happens upon exposure to oxidant stress • The most common triggers are infections, in which oxygen-derived free radicals are produced by activated leukocytes • Many infections can trigger hemolysis; viral hepatitis, pneumonia, and typhoid fever • The other important initiators are drugs and certain foods • Most important drugs are the antimalarials (e.g., primaquine and chloroquine), sulfonamides, nitrofurantoins • Some drugs cause hemolysis only in individuals with the more severe Mediterranean variant. • The most frequently cited food is the fava bean (Favism) • Uncommonly, G6PD deficiency presents as neonatal jaundice or a chronic low-grade hemolytic anemia in the absence of infection or known environmental triggers
Clinical features • Majority of patients are asymptomatic, anemia develops when the enzyme level drops below 20% of normal activity • Hemolytic crisis appear 2-3 days after exposure to oxidant • Only old RBCs hemolize, HB level drops, RBCs appear normochromicnormocytic, patients have bone pain • Chronic hemolysis (splenomegaly and GB stones) are absent • G6PD-A usually is self-limited • G6PD-Mediterranian has more severe crisis, might need blood transfusion • Recovery is associated with reticulocytosis • Dx: enzyme assay (measure conversion to NAPDH)
Pyrovatekinase deficiency • AR inheritance • PK is an enzyme in the anaerobic glycolysis pathway (main pathway in RBCs) • PK deficiency causes decreased ATP level which is essential for cell membrane pumps • Intracellular Na accumulates, causing swelling of RBCs and rigidity • Spleen clears abnormal shaped RBCs • 2,3 diphosphoglycerate (DPG) level increases inside RBCs, facilitating O2 release, ameliorating the anemia
Clinical • Degree of anemia varies according to type of mutation, ranging from neonatal jaundice to anemia presenting in adulthood with jaundice, GB stones and splenomegaly • Anemia is exacerbated by stress • Blood film shows NN anemia, variable reticulocytosis, anisopoikelocytosis • Diagnosis: enzyme assay • Treatment: splenectomy
Paroxysmal Nocturnal Hematuria • Acquired disease • Normally, proteins are anchored into the lipid bilayer in two ways. Most have a hydrophobic region that spans the cell membrane; these are called transmembrane proteins. The others are attached to the cell membrane through a covalent linkage to a specialized phospholipid called glycosylphosphatidylinositol (GPI) • In PNH, there is a mutation in the phosphatidylinositolglycan complementation group A gene (PIGA), which synthesizes GPI • Thus, GPI and their normally anchored proteins are absent • Because the causative mutations occur in a hematopoietic stem cell, all of its clonal progeny (red cells, white cells, and platelets) are deficient in GPI-linked proteins
Patholophysiology • Normal individuals harbor small numbers of bone marrow cells with PIGA mutations • In PNH, autoimmune reaction occurs against normal clones resulting in predominance of GPI-deficient clone • PNH blood cells are deficient in three GPI-linked proteins that regulate complement activity: (1) decay-accelerating factor, or CD55; (2) membrane inhibitor of reactive lysis, or CD59; and (3) C8 binding protein. Of these factors, the most important is CD59, a potent inhibitor of C3 convertase that prevents the spontaneous activation of the alternative complement pathway
Clinical features • Red cells, platelets, and granulocytes deficient in these GPI-linked factors are abnormally susceptible to lysis or injury by complement. In red cells this manifests as intravascular hemolysis, which is caused by the C5b-C9 membrane attack complex • The hemolysis is intravascular, paroxysmal and nocturnal in only 25% of cases; chronic hemolysis without dramatic hemoglobinuria is more typical. The tendency for red cells to lyse at night is explained by a slight decrease in blood pH during sleep, which increases the activity of complement • Thrombosis is the leading cause of death in PNH. About 40% of patients suffer from venous thrombosis, often involving the hepatic, portal, or cerebral veins. Autolysis of some platelets causes aggregation of others secondary to released prothrombotic factors • In severe cases, pancytopenia develops • About 5% to 10% of patients eventually develop acute myeloid leukemia or a myelodysplastic syndrome, possibly because hematopoietic stem cells have suffered some type of genetic damage.
Autoimmune hemolytic anemia • A group of anemias in which an abnormal immunoglobulin is attached to RBC membrane causing damage and lysis • Direct Coombs antiglobulin test: the patient's RBCs are mixed with sera containing antibodies that are specific for human immunoglobulin. If either immunoglobulin is present on the surface of the red cells, the multivalent antibodies cause agglutination, which is easily appreciated visually as clumping • Indirect Coombs antiglobulin test, the patient's serum is tested for its ability to agglutinate commercially available red cells bearing particular defined antigens
Warm Antibody Type • 70% of immunohemolytic anemia. • 50% are idiopathic (primary); the others are related to a predisposing condition or exposure to a drug. • Most causative antibodies are of the IgG class; less commonly, IgA antibodies • A common target is the Rh antigen on RBCs • The red cell hemolysis is mostly extravascular. IgG-coated red cells bind to Fc receptors on phagocytes, which remove red cell membrane during "partial" phagocytosis. As in hereditary spherocytosis, the loss of membrane converts the red cells to spherocytes, which are sequestered and removed in the spleen. Moderate splenomegaly due to hyperplasia of splenic phagocytes is usually seen
Drug induced hemolytic anemia • Antigenic drugs. In this setting hemolysis usually follows large, intravenous doses of the offending drug and occurs 1 to 2 weeks after therapy is initiated. These drugs, like penicillin and cephalosporins, bind to the red cell membrane and are recognized by anti-drug antibodies. Sometimes the antibodies bind only to the drug, as in penicillin-induced hemolysis. In other cases, such as in quinidine-induced hemolysis, the antibodies recognize a complex of the drug and a membrane protein. The responsible antibodies sometimes fix complement and cause intravascular hemolysis, but more often they act as opsonins that promote extravascularhemolysis within phagocytes • Tolerance-breaking drugs. These drugs, of which the antihypertensive agent α-methyldopa is the prototype, induce in some unknown manner the production of antibodies against red cell antigens, particularly the Rh blood group antigens. About 10% of patients taking α-methyldopa develop autoantibodies, as assessed by the direct Coombs test, and roughly 1% develop clinically significant hemolysis
Cold Agglutinin Type • This form of immunohemolytic anemia is caused by IgM antibodies that bind red cells avidly at low temperatures (0°-4°C). It is less common than warm antibody immunohemolytic anemia, accounting for 15% to 30% of cases • Cold agglutinin antibodies sometimes appear transiently following certain infections, such as with Mycoplasmapneumoniae, Epstein-Barr virus, cytomegalovirus, influenza virus, and human immunodeficiency virus (HIV). In these settings the disorder is self-limited and the antibodies rarely induce clinically important hemolysis. Chronic cold agglutinin immunohemolytic anemia occurs in association with certain B-cell neoplasms or as an idiopathic condition. • Clinical symptoms result from binding of IgM to red cells in vascular beds where the temperature may fall below 30°C, such as in exposed fingers, toes, and ears. IgM binding agglutinates red cells and fixes complement rapidly. As the blood recirculates and warms, IgM is released, usually before complement-mediated hemolysis can occur. However, the transient interaction with IgM is sufficient to deposit sublytic quantities of C3b, an excellent opsonin, which leads to the removal of affected red cells by phagocytes in the spleen, liver, and bone marrow. The hemolysis is of variable severity
Cold Hemolysin Type • Cold hemolysins are autoantibodies responsible for an unusual entity known as paroxysmal cold hemoglobinuria • This rare disorder causes substantial, sometimes fatal, intravascular hemolysis and hemoglobinuria • The autoantibodies are IgGs that bind to the P blood group antigen on the red cell surface in cool, peripheral regions of the body. Complement-mediated lysis occurs when the cells recirculate to warm central regions, since the complement cascade functions more efficiently at 37°C • Most cases are seen in children following viral infections; in this setting the disorder is transient, and most of those affected recover within 1 month.
Hemolytic Anemia Resulting from Trauma to Red Cells • Physical damage to RBCs • Cardiac valve prosthesis • Microangiopathic disease (disseminated intravascular coagulation DIC, thrombotic thrombocytopenic purpura (TTP), hemolytic-uremic syndrome (HUS), malignant hypertension, systemic lupus erythematosus, and disseminated cancer): aggregates of fibrin and platelets causes damage to RBCs • RBCs appear as fragments (schistocytes)
Normal Hemoglobin Structure • Two pairs of globin chains with a haem group attached. • 7 chains are synthesized in normal subjects: 4 embryonic: Hg Gower 1,2 Hg Portland 1,2. Hg F (fetal), Hg A, Hg A2 • The individual chains synthesized in postnatal life are designated α, β, γ, and δ • Hg A has two α chains and two β chains (α2 β2) • Hg A2 has two α chains and two δ chains (α2 δ2), 1.5-3% • Hg F has two α chains and two γ chains (α2 γ2), 1%
* α Chain synthesis is directed by two α genes, α 1 and α 2, on chromosome 16 * β and δ chain synthesis by single β and δ genes on chromosome 11 * γ Chain synthesis is directed by two genes, Gγ and Aγ, also on chromosome 11 Genes controling Hg synthesis
Thalassemia • The thalassemia syndromes are a heterogeneous group of disorders caused by inherited mutations that decrease the synthesis of adult hemoglobin, HgA (α2β2) • Endemic in Middle East, tropical Africa, India, Asia • β-Thalassemia is caused by deficient synthesis of β chains, whereas α-thalassemia is caused by deficient synthesis of α chains • The hematologic consequences of diminished synthesis of one globin chain stem not only from hemoglobin deficiency but also from a relative excess of the other globin chain, particularly in β-thalassemia
β-Thalassemias • caused by mutations that diminish the synthesis of β-globin chains • β0mutations, associated with absent β-globin synthesis • β+mutations, characterized by reduced (but detectable) β-globin synthesis • 100 different causative mutations, mostly consisting of point mutations
Types of mutations • Splicing mutations: most common cause of β+-thalassemia. Most of these mutations lie within introns, while a few are located within exons. Some of these mutations destroy the normal RNA splice junctions and completely prevent the production of normal β-globin mRNA, resulting in β0-thalassemia • Promoter region mutations. These mutations reduce transcription by 75% to 80%. Some normal β-globin is synthesized; thus, these mutations are associated with β+-thalassemia. • Chain terminator mutations. These are the most common cause of β0-thalassemia. Two subtypes of mutations fall into this category. The most common type creates a new stop codon within an exon; the second introduces small insertions or deletions that shift the mRNA reading frames, Both block translation and prevent the synthesis of any functional β-globin
Pathophysiology • The deficit in HgA synthesis produces "underhemoglobinized" hypochromic, microcytic red cells with subnormal oxygen transport capacity • Diminished survival of red cells and their precursors, which results from the imbalance in α- and β-globin synthesis. Unpaired α chains precipitate within red cell precursors, forming insoluble inclusions, which damage cell membrane and results in cell death in RBC precursors (Ineffective erythropoiesis) • Those red cells that are released from the marrow also bear inclusions and membrane damage and are prone to splenic sequestration and extravascular hemolysis