Download
1 / 40
430 likes | 1.08k Views
Anthrax. Bacillus anthracis. Microbiology. Bacillus anthracis. Microbiology. Bacillus anthracis Aerobic, large Gram positive bacillus. Microbiology. Bacillus anthracis Aerobic, large Gram positive bacillus Non-motile, non-hemolytic. Microbiology. Bacillus anthracis

E N D
Anthrax Bacillus anthracis
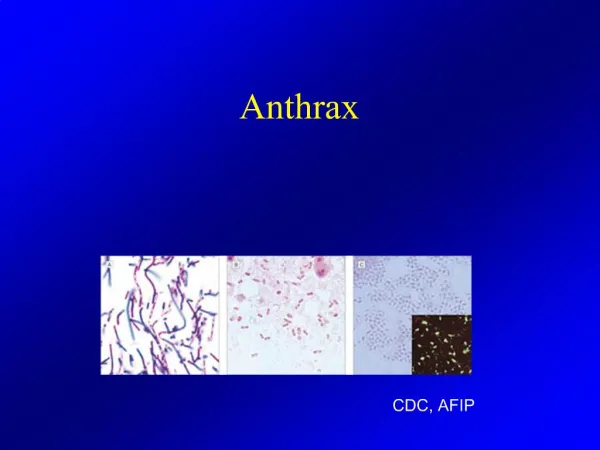
Microbiology • Bacillus anthracis
Microbiology • Bacillus anthracis • Aerobic, large Gram positive bacillus
Microbiology • Bacillus anthracis • Aerobic, large Gram positive bacillus • Non-motile, non-hemolytic
Microbiology • Bacillus anthracis • Aerobic, large Gram positive bacillus • Non-motile, non-hemolytic
Microbiology • Bacillus anthracis • Aerobic, large Gram positive bacillus • Non-motile, non-hemolytic • Forms hardy spores • Triggered by harsh environment • Inert but infectious • 1m size
Diagnosis of Anthrax • High index of suspicion necessary • No readily available rapid test • Gold Standard - culture blood, fluids • Prior to antibiotics
Diagnosis of Anthrax • High index of suspicion necessary • No readily available rapid test • Gold Standard - culture blood, fluids • Prior to antibiotics • Confirmation by reference labs • PCR, special stains, serology, etc
Diagnosis of Anthrax • High index of suspicion necessary • No readily available rapid test • Gold Standard - culture blood, fluids • Prior to antibiotics • Confirmation by reference labs • PCR, special stains, serology, etc • Nasal swabs not a diagnostic tool
Treatment • Hospitalization • IV antibiotics • Empiric until sensitivities known • Intensive supportive care • Electrolyte and acid-base imbalances • Mechanical ventilation • Hemodynamic support
Treatment • Hospitalization • IV antibiotics • Empiric until sensitivities known • Intensive supportive care • Electrolyte and acid-base imbalances • Mechanical ventilation • Hemodynamic support • Steroids • Consider for severe disease
Treatment • Empiric therapy for inhalational (Adults)
Treatment • Empiric therapy for inhalational (Adults) • Ciprofloxacin 400 mg IV q12° OR Doxycycline 100 mg IV q12° AND One or two other antibiotics - clindamycin - penicillin - vancomycin - chloramphenicol - rifampin - imipenem
Treatment • Empiric therapy for inhalational (Adults) • Ciprofloxacin 400 mg IV q12° OR Doxycycline 100 mg IV q12° AND One or two other antibiotics - clindamycin - penicillin - vancomycin - chloramphenicol - rifampin - imipenem • Avoid macrolides, cephalosporins, sulfa
Treatment • Empiric therapy for inhalational (Children) Ciprofloxacin 10-15 mg/kg/d IV q12° (max 1 g/d)
Treatment • Empiric therapy for inhalational (Children) Ciprofloxacin 10-15 mg/kg/d IV q12° (max 1 g/d) OR Doxycycline 2.2 mg/kg IV q12° (adult dose >8yo/45 kg)
Treatment • Empiric therapy for inhalational (Children) Ciprofloxacin 10-15 mg/kg/d IV q12° (max 1 g/d) OR Doxycycline 2.2 mg/kg IV q12° (adult dose >8yo/45 kg) AND One or two antibiotics (same as adult)
Treatment • Empiric therapy for inhalational(Children) Ciprofloxacin 10-15 mg/kg/d IV q12° (max 1 g/d) OR Doxycycline 2.2 mg/kg IV q12° (adult dose >8yo/45 kg) AND One or two antibiotics (same as adult) • Weigh risks (arthropathy, dental enamel)
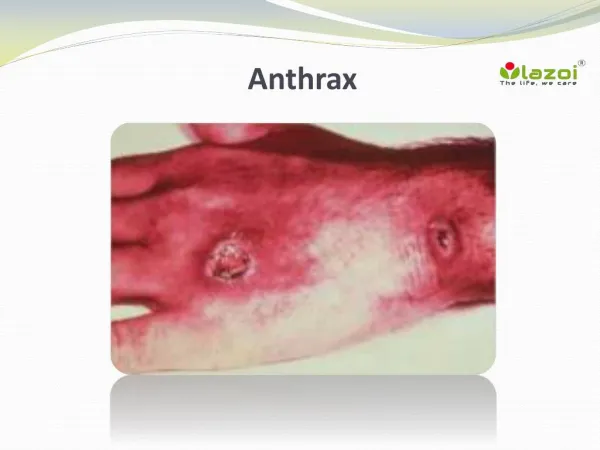
Treatment • Empiric therapy for cutaneous • Same as inhalational regimen if: • Systemic disease • Extensive edema • Head/neck lesions
Treatment • Empiric therapy for cutaneous • Same as inhalational regimen if: • Systemic disease • Extensive edema • Head/neck lesions • Localized cutaneous • Ciprofloxacin 500mg po bid OR • Doxycycline 100mg po bid
Treatment • Empiric therapy for cutaneous • Same as inhalational regimen if: • Systemic disease • Extensive edema • Head/neck lesions • Localized cutaneous • Ciprofloxacin 500mg po bid OR • Doxycycline 100mg po bid • Empiric therapy for GI • Same as inhalational
Treatment • Antibiotic therapy – all forms • Adjust per sensitivities • Duration • 60 days - delayed spore germination • Follow closely after cessation
Treatment • Antibiotic therapy – all forms • Adjust per sensitivities • Duration • 60 days - delayed spore germination • Follow closely after cessation • Switch to oral • Clinical improvement, able to tolerate po • 1 or 2 drugs including cipro or doxy initially • Children can complete course with amoxicillin
Treatment • Antibiotic therapy – all forms • No role for vaccine in treatment
Post-Exposure Prophylaxis • Indications • Exposure to anthrax spores • Not for contacts of cases
Post-Exposure Prophylaxis • Indications • Exposure to anthrax spores • Not for contacts of cases • Oral antibiotics • Ciprofloxacin 500mg po bid OR • Doxycycline 100mg po bid • Duration 60-100 days
Post-Exposure Prophylaxis • Indications • Exposure to anthrax spores • Not for contacts of cases • Oral antibiotics • Ciprofloxacin 500mg po bid OR • Doxycycline 100mg po bid • Duration 60-100 days • +/- Vaccination • May reduce PEP duration to 30 days
Vaccination • Limited supply
Vaccination • Limited supply • Inactivated, cell-free vaccine
Vaccination • Limited supply • Inactivated, cell-free vaccine • Effective • >95% animals vs. inhalational • Protective for humans vs. cutaneous
Vaccination • Limited supply • Inactivated, cell-free vaccine • Effective • >95% animals vs. inhalational • Protective for humans vs. cutaneous • Well-tolerated • Uncommon adverse effects • No reported deaths
Infection Control • Person-to-person transmission • None for inhalational • Rarely reported for cutaneous
Infection Control • Person-to-person transmission • None for inhalational • Rarely reported for cutaneous • Patient handling • Standard precautions • Gloves for draining lesions
Infection Control • Person-to-person transmission • None for inhalational • Rarely reported for cutaneous • Patient handling • Standard precautions • Gloves for draining lesions • Laboratory safety • BSL-2 for clinical specimens • BSL-3 for environmental or large volume