Download
1 / 36
360 likes | 473 Views
Transfusion-Related Challenges in Rural Alaska. JAMES J. TIESINGA, MD Laboratory Medical Director Alaska Tribal Health System. OVERVIEW. Criteria for blood utilization review Emergency release Final disposition Documentation Operational challenges / staff turnover

E N D
Transfusion-Related Challenges in Rural Alaska JAMES J. TIESINGA, MD Laboratory Medical Director Alaska Tribal Health System
OVERVIEW • Criteria for blood utilization review • Emergency release • Final disposition • Documentation • Operational challenges / staff turnover • Impact of Quality Management
BLOOD UTILIZATION REVIEW • Ordering • Handling • Dispensing • Administration • Monitoring
EAST STUDY • A “restrictive” strategy of red cell transfusion, based on a transfusion threshold of Hb < 7 g/dL, is as effective as a “liberal” transfusion strategy, based on a transfusion threshold of Hb < 10 g/dL, in critically ill patients with hemodynamically stable anemia.
EAST Continued • Consider transfusion of Hb < 7 g/dL in critically ill patients with stable cardiac disease. “There is no benefit of a “liberal” transfusion strategy in critically ill patients with stable cardiac disease.” And, • RBC transfusion should not be considered as an absolute method to improve tissue oxygen consumption in critically ill patients.
Criteria for transfusion: • Hemoglobin of < 8 gm/dl or Hematocrit of < 24% • Hemoglobin between 8-10gm/dl and one of the following is present: • Acutely bleeding • Trauma or burn patient • >65 years old • A drop of 2 gm/dl Hgb or more in 12 hours • Coronary artery disease, chronic lung disease, cerebrovascular disease, or pregnant • Before or during radiation or chemotherapy • Post-transfusion Hgb/Hct not in excess of 12 gm/dl/ 36% when no pre-transfusion values are available.
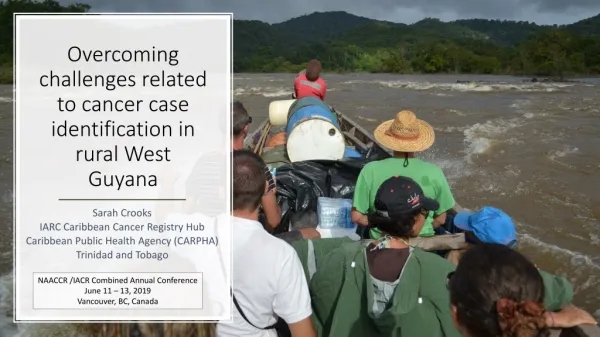
AIR MEDICAL TRANSPORT • limited availability of emergency intervention services in remote facilities, • air medical transport has become crucial for access to definitive care
Conclusions Overutilization is not a significant issue A more conservative transfusion criteria is unlikely to impact in-house or Air Transport practice Decision to Air Transport depend on clinical criteria other than the degree of anemia Air Transport transfusion may reflect concern for delays and distances involved Gastrointestinal bleeding model may approximate Air Transport practice better than trauma model
EMERGENCY RELEASE OF BLOOD • Review laboratory records • Determine Rh type and number of units in inventory • Release of O(+) blood to women • Retrospective Crossmatch • Notification • Documentation
Transfusion-Related Documentation Frequent staff turnover – a chronic problem in remote facilities, The use of rotating TDYs or Locums among Laboratory staff, nurses, and physicians, and The use of some staff, such as air medical transport crew, who may not be employees of your organization, which leads to loss of document control.
Documenting Final Disposition The Laboratory releasing the blood is responsible for documenting its final disposition, that is, whether or not it was transfused. It is the responsibility of the Laboratory that issued the unit to ensure air medical transport documents on the TRF whether or not the unit was transfused en route. Documentation of final disposition is essential for appropriate management of clinical transfusion risks.
Documenting Vital Signs The Laboratory is responsible for maintaining appropriate standards of practice for transfusion across all departments in your organization. If air transport personnel and / or EMS crew is employed by your hospital organization, then the Laboratory is responsible for ensuring air medical transport completes its documentation in accordance with your Laboratory’s procedures.
Training and Competency Blood should never be released to nursing staff or air medical transport crew unless your laboratory has documented training and competency of these nurses or crew on how to check out and transfuse blood according to your Laboratory’s procedures. Lippincott / Elsevier Transfusion-Related Nursing Procedures: Generally a really BAD idea!
Temperature Control Hemotemp sticker or similar device should be applied to every unit released to air medical transport to ensure appropriate temperature was maintained throughout transport of the units. Standards require temperature to be taken on all units of blood prior to return to inventory to ensure these units have not exceeded 10 degrees.
Quality Management To successfully address transfusion-related challenges effectively, including those under discussion, the Laboratory must have a plan in place defining levels of authority and responsibility for all personnel, ensuring effective training and competency, maintaining processes for document control, managing occurrences and process improvements, and supporting other fundamentals of effective quality management.
Maniilaq Health Center Kotzebue, AK Maniilaq Health Center (MHC) is located in Kotzebue, Northwest Alaska, 30 miles above the Arctic Circle. It is part of a System (MHS) owned and operated by the Tribal Health Organization of Maniilaq Association that serves the 3,500 residents of the native village of Kotzebue, Alaska, and the estimated 8,000 residents of the 10 villages of the Northwest Arctic Borough and Point Hope (North Slope Borough).
Background:Service to Native Communities MHS provides laboratory services to the residents of Kotzebue and the 11 surrounding villages. MHC Laboratory oversees the transfusion of packed red blood cells (PRBC) in these 11 villages.
Blood Transfusion in the Arctic • Providing transfusion services in rural Alaska presents significant challenges in assuring quality of care and patient safety. • These challenges are primarily related to staff turnover, communication among caregivers, and overall coordination of care.
Coordination of Care Staff Turnover Nursing Training and Competency Nursing Documents • Staffcoo Physician Consent Low Volume Medical Flight Nursing Inventory Laboratory Training and Competency Laboratory Documents
Assessment: August 2007 to April 2010 • MHC Laboratory performed quarterly blood utilization review consisting of assessment of laboratory documents and patient charts for all transfusions. • Blood utilization averaged 6 units packed red cells / month during this period (N=187). • Significant non-conformances in documentation: • defined as violation of organizational procedures and/or • failure to follow accreditation standards pertaining to transfusion records; • variance rate was 86% of all transfusions (N=160).
Quality Tools Initiated a comprehensive quality improvement project to address these challenges. This project employed key quality tools: • Brainstorming • Pareto charting • Cause and effect assessment • Task sharing
Clarified / simplified forms • Implementation of simplified forms and real-time supervision of documentation proved most effective in reducing errors.
Developed interdepartmental corrective actions • Proactive corrective actions • Intradepartmental coordination process involved alerting a Nurse Educator/Manager prior to each transfusion, thereby allowing real-time oversight and review of documentation and timely remedial training.
Challenges in Microbiology Accuracy of data used to construct antibiograms. Appropriateness of sensitivity reports.
POC i-STAT Troponin Testing Moderate complexity. Must verify the accuracy of the analyte result obtained at least twice annually, using split sample testing or proficiency testing (non-regulated analyte). Perform and document calibration verification at least once every 6 months. Perform correlation between test results using different methodologies, instruments, or testing sites at least once every 6 months. Verify the refrigerator does not exceed 2-8°C. Verify room temperature does not exceed 30°C. Verify cartridge does not exceed 14 days at room temperature. Keep package inserts and manufacturer’s assay sheets for 2 years.
Miscellaneous LIS Make sure: Printout (downtime) RRs match the LIS. Lab results are CLIA compliant and include name / address of referral laboratories. Periodically update your LIS test environment. Periodically verify the accuracy of data transfer across separate components of your LIS (Micro vs. Core), and between your LIS and EHR. Periodically verify the accuracy of LIS calculations.