Download
1 / 43
4.9k likes | 13.9k Views
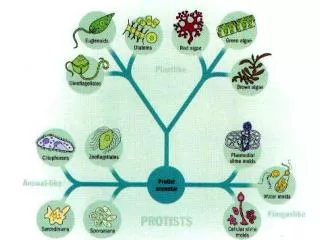
The Protozoa . Introduction: The Phylum Protozoa is classified into four subdivisions according to the methods of locomotion. The amoebae (Sarcodina) move by means of pseudopodia. The flagellates (Mastigophora) typically move by long, whiplike flagellae.

E N D
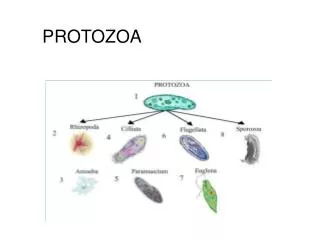
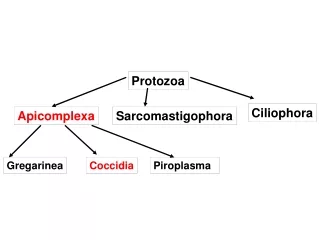
The Protozoa Introduction: The Phylum Protozoa is classified into four subdivisions according to the methods of locomotion. • The amoebae (Sarcodina) move by means of pseudopodia. • The flagellates (Mastigophora) typically move by long, whiplike flagellae. • The ciliates (Ciliata) are propelled by rows of cilia that beat with a synchronized wavelike motion. • The sporozoans (Sporozoa) lack specialized organelles of motility.
The Protozoa General: • There are about 45,000 protozoan species; around 8000 are parasitic, and around 25 species are important to humans. • Diagnosis - must learn to differentiate between the harmless and the medically important. This is most often based upon the morphology of respective organisms. • Transmission - mostly person-to-person, via fecal-oral route; fecally contaminated food or water; other means include sexual transmission, insect bites or insect feces.
The Protozoa General: • Trophozoite - the motile vegetative stage; multiplies via binary fission; colonizes host. • Cyst - the inactive, non-motile, infective stage; survives the environment due to the presence of a cyst wall. Cysts do not multiply, however, some organisms divide within the cyst wall.
The Protozoa Diagnostic Features: • Nuclear structure - important in species differentiation. • Size - helpful in identifying organisms; must have calibrated objectives on the microscope in order to measure accurately. • Cytoplasmic inclusions - chromatoid bars (coalesced RNA); red blood cells; food vacuoles containing bacteria, yeast, etc. • Appearance of cytoplasm - smooth & clean or vacuolated. • Type of motility - directional or non-directional; sluggish or fast.
The Protozoa Nuclear Structure: • Chromatin - nuclear DNA. Present as “peripheral” chromatin and the karyosome. • Karyosome - a small mass of chromatin within the nuclear space. Also called “endosome” or “centrosome.” • Peripheral Chromatin - chromatin adhering to the nuclear membrane. • Nuclear membrane - membrane surrounding all nuclear material. Chromatoid body or “bar” - coalesced RNA within the cytoplasm of the cyst stage.
The Protozoa Intestinal Protozoa -The Amoebae General Life cycle - • The definitive host ingests the infective cyst stage from fecal contamination in environment. • The cyst passes into the small intestine & excystation occurs with transformation to the trophozoite stage. • Trophozoites colonize the host, multiplying asexually via binary fission. They can remain near the lumen (non-pathogens) or invade the wall of the intestine & multiply (pathogens). • Cysts and trophozoites are passed in the feces of the infected host.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba histolytica • Epidemiology - Occurs worldwide; the highest incidence and prevalence is in areas with poor sanitation. • Pathology and Clinical Manifestations - the most pathogenic of all; causes amoebic dysentery; can become extra-intestinal; can be fatal. Hepatic abscess is the most common and dangerous complication. • Chronic infections may last for years; often confused with colitis, cancer. • Distribution - worldwide, mostly in tropics and sub-tropics.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba histolytica • Morphology & Laboratory Identification - trophozoites range 12 to 30 microns in diameter; nucleus has an even distribution of peripheral chromatin and a small, compact, centrally located karyosome; cytoplasm is smooth and granular; inclusions, if present, are red blood cells; cysts range 10 to 20 microns in diameter and contains four nuclei when mature. Cigar-shaped chromatoid bars may be present in some cysts.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba hartmanni • Epidemiology - similar to E. histolytica • Formerly called the “small race” of Entamoeba histolytica. • Technologists must be able to differentiate this organism from E. histolytica because E. hartmanni is non-pathogenic.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba hartmanni • Morphology & Laboratory Identification - This organism is morphologically similar to E. histolytica. The difference lies in the sizes of the respective organisms. Trophozoites will measure less than 12 microns, while cysts will measure less than 10 microns.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba coli • Significance - this is a harmless commensal; must be differentiated from pathogens. • Morphology - trophozoites range from 10 to 35 microns in diameter; cysts range from 10 to 30 microns in diameter and contain 8 to 16 nuclei when mature; the nucleus exhibits an eccentric karyosome with irregular, coarse chromatin. The cytoplasm is heavily vacuolated, containing yeast, bacteria, and debris.
The Protozoa Intestinal Protozoa -The Amoebae Entamoeba gingivalis • Infective site - the mouth; the organism thrives in diseased gums, but is not considered a causal agent. It is destroyed in stomach if swallowed. • Transmission - contact with fomites (drinking glasses, eating utensils, etc.); kissing. • Morphology - resembles E. histolytica, but has no cyst stage. It is the only species which ingests leucocytes.
The Protozoa Intestinal Protozoa -The Amoebae Endolimax nana • Occurrence - occurs in about 14% of the US population; 21% worldwide. • Pathogenicity - none. • Morphology - trophozoites range from 5 to 10 microns in diameter. The nucleus contains a large, blot-like karyosome; there is little or no peripheral chromatin. Cysts are usually sub-oval, measuring 4 to 6 by 6 to 10 microns.
The Protozoa Intestinal Protozoa -The Amoebae Iodamoeba butschlii • Pathogenicity - none. • Morphology - the cyst is often called the “iodine cyst” due to the presence of a large glycogen vacuole which stains dark brown with iodine.
The Protozoa Tissue Dwelling Amoebae Naegleria fowleri • Classification - an ameboflagellate; a free-living organism alternating between amoeboid and flagellated forms; only the amoeboid form is found in tissues. • Life cycle - the amoeba gains entry via the nasal mucosa, usually during a swimming event; it moves along the olfactory nerve, gaining access to the brain via the cribriform plate. Cases are invariably fatal. Infections do not spread from person-to-person. Naegleria fowleri trophozoite in CSF
The Protozoa Tissue Dwelling Amoebae Naegleria fowleri • Symptoms - Dramatic and rapidly progressive. Headache, fever, nausea & vomiting occur within 1 to 2 days. Meningoencephalitis, irrational behavior, coma & death usually occur within 9 days of exposure. • Diagnosis - Usually made at autopsy. CSF contain motile amoebae. Early diagnosis is critical. Amoebae in CSF specimens can be cultured on non-nutrient agar containing bacteria.
The Protozoa Tissue Dwelling Amoebae Acanthamoeba spp. • Life cycle - also a free-living amoeba. The amoeba reaches the brain hematogenously after entering a wound or lesion on the skin. More commonly, the organism is associated with getting into eyes via contaminated or homemade cleaning solutions. • Symptoms - slow onset (10 or more days). Presents as chronic, granulomatous lesions in brain. In eye lesions, the infection resembles a herpes virus infection. • Acanthamoeba keratitis - associated with users of extended-wear contact lenses.
The Protozoa Superclass Mastigophora - the flagellates. Inhabit the mouth, bloodstream, gastrointestinal, or urogenital tracts. Morphological Characteristics • Flagellum(ae) - organelles of locomotion; an extension of ectoplasm; moves with a whip-like motion. • Axostyle - a supporting mechanism, a rod-shaped structure; not all flagellates have these. • Undulating membrane - a protoplasmic membrane with a flagellar rim extending out like a fin along the outer edge of the body of some flagellates. • Costa - a thin, firm rod-like structure running along the base of the undulating membrane. • Cytosome - a rudimentary mouth; also referred to as a gullet.
The Protozoa Superclass Mastigophora - the flagellates. Identification of a flagellate is based upon: • Size. • Shape. • Motility. • Number and morphology of nuclei. • Number and location of flagellae. • Location in the body of the host.
The Protozoa Intestinal flagellates Giardia lamblia • Most common protozoan parasite in the U.S.A. • Life cycle - man ingests cysts from fecally contaminated environment; the organism excysts in the upper intestine; trophozoites multiply and attach to the intestinal mucosa; often enter the gall bladder. Trophozoites and cysts are passed in the feces. • Diagnosis - identification of cysts or trophozoites in stool specimens or duodenal contents.
The Protozoa Intestinal flagellates Giardia lamblia Morphology - very distinctive. Dorsal-ventrally flattened, and Bi-laterally symmetrical. • Cyst - 9 x 12 micrometers and contain 2 to 4 nuclei; parabasal bodies are present. • Trophozoite - Four pairs of flagella - one pair located anterior, two pair located ventrally, and one pair located posteriorly. An axostyle and parabasal bodies are present.
The Protozoa Intestinal flagellates Giardia lamblia • Epidemiology - prevalence 1 to 30%, common in children’s day care centers; can be transmitted in water. Sexual transmission has been well documented. • Pathology and Clinical Manifestations - symptoms can be severe; diarrhea, foul-smelling, greasy, mucus-laden stools, flatulence, nausea, cramps. Most infections are asymptomatic; chronic cases experience weight loss, malabsorption of fat, protein, folic acid, and fat-soluble vitamins.
The Protozoa Intestinal flagellates Dientamoeba fragilis • General - Formerly classified as an amoeba; electron microscopy and immunological studies have suggested a flagellate nature. • Laboratory diagnosis - detection of bi-nucleated trophozoites; fragmented karyosomes consisting of 4 to 8 granules of chromatin.
The Protozoa Intestinal flagellates Dientamoeba fragilis Diagnostic stage - the trophozoite in feces. There is no cyst stage. • Morphology - 1 or 2 nuclei, with little or no peripheral chromatin; karyosome is divided into 4 to 8 distinct granules. • May rarely ingest rbc’s.
The Protozoa Intestinal flagellates Dientamoeba fragilis • Pathology - infection is usually asymptomatic; can be associated with diarrhea, anorexia, abdominal pain. • Association with pinworm - the organism may be transmitted from host to host within the egg of Enterobius vermicularis. • Distribution - worldwide, there is a 1% to 20% prevalence.
The Protozoa Intestinal flagellates Chilomastix mesnili • A non-pathogen - must be differentiated from Giardia. • Found in cecum and colon. • Transmission - by ingestion of mature cysts.
The Protozoa Intestinal flagellates Chilomastix mesnili Morphology - • Trophozoite - 4 flagella (3 anterior, 1 associated with the cytostome; one nucleus, always located anteriorly. • Cyst - lemon shape; 1 nucleus; cytostome may be seen.
The Protozoa The Trichomonads Characteristics - • Undulating membrane - protoplasmic membrane with flagellar rim extending out like a fin along outer edge of body. • Flagella - several in a tuft, provides locomotion. • Axostyle - functions for support. • Costa - firm rod-like structure running along base of the undulating membrane. • Cytostome - rudimentary mouth.
The Protozoa The Trichomonads Trichomonas hominis • Commensal - must differentiate from pathogens. • Transmission - direct person-to-person fecal transmission; no cyst stage. • Morphology - “arc-shaped” exhibits a wobbly, jerky, motility. • Must differentiate from T. vaginalis - in instances where feces is contaminated with urine.
The Protozoa The Trichomonads Trichomonas vaginalis • Life cycle - trophozoite lives in the vagina, urethra, epididymis, and prostate; multiplies via longitudinal fission; no cyst stage. • Mode of infection - sexual intercourse or fomites. • Diagnosis - identification of trophozoites in body fluids (wet mounts of discharges) or on PAP smears.
The Protozoa The Trichomonads Trichomonas vaginalis • Pathology - Females: vaginal discharge; burning, Itching, or chafing. Frequency of urination or dysuria. Males: frequently asymptomatic. If the prostate is involved, the patient may develop discharge, dysuria, and enlargement of prostate with tenderness. • Morphology - has an axostyle and short undulating membrane that extends less than half the body length; 4 flagellae.
The Protozoa Class Ciliophora - The Ciliates Balantidium coli • Epidemiology - Rarely found in USA. This is the only ciliate parasite of humans. • Largest parasitic protozoan - trophozoite is 30-120 x 25-125 microns; the cyst averages 50 - 70 microns in diameter. • Life cycle - The cyst is ingested via fecal contamination in environment; cysts excyst in the small intestine; trophozoites migrate to large intestine.
The Protozoa Class Ciliophora - The Ciliates Balantidium coli • Pathology & Symptoms - Many infections are asymptomatic, organism feeding on bacteria at surface of mucosa. Severe infections - with the aid of hyaluronidase, the organism burrows into submucosa, producing ulcers. Symptoms - dysentery, abdominal pain, nausea & vomiting, fever, headache. • Diagnosis - Diagnosed by observing cysts & trophozoites in fecal samples.
The Protozoa Class Ciliophora - The Ciliates Balantidium coli • Morphology - Large, oval shape; two nuclei, 1 large kidney shaped (macronucleus) & 1 small micronucleus (micronucleus not often seen); body surface covered by longitudinal rows of cilia; cytostome present. • Primary animal reservoir - pigs, monkeys.
The Protozoa Intestinal Coccidia General - • Organisms infecting humans include Isospora, Sarcocystis, Cryptosporidium, Cyclospora & Toxoplasma. • Some have 2-host life cycle. • Sexual & asexual reproduction - Schizogony - asexual binary fission; Sporogony - sexual reproduction. • Diagnostic stages are often difficult to locate. Acid fast stains are used to visualize. Oocysts do not stain with iodine or permanent stains like trichrome.
The Protozoa Intestinal Coccidia Sarcocystissuihominis Sarcocystis bovihominis Sarcocystis lindemanni • Pathology - Sarcocystis bovihominis & S. suihominis are intestinal infections. Sarcocystis lindemanni is a muscle infection. • Humans are definitive hosts for S. suihominis & bovihominis; intermediate hosts are pig (sui-) and cow (bovi-); humans are intermediate hosts for S. lindemanni; the definitive host is unknown. • Infective stage - sarcocysts in meat (intestinal); ingestion of oocysts from animal feces (muscle).
The Protozoa Intestinal Coccidia Isospora belli • Definitive host - humans. • Schizogony - takes place upon initial infection when sporozoites invade the intestinal epithelium and multiply. Sporogony - progeny of asexual reproduction initiate development into gametes (male & female); fertilized gametes develop into oocysts which are passed as the infectious stage in the feces.
The Protozoa Intestinal Coccidia Isospora belli • Diagnostic/infective stage - mature oocyst - contains two sporocysts, each of which contain four sporozoites (do not stain with iodine). • Intermediate hosts - none. • Pathology - ranges from asymptomatic to acute, severe dysentery.
The Protozoa Intestinal Coccidia Cryptosporidium parvum • Site of infection - primarily an intestinal infection, can become systemic in AIDS patients. • Originally considered an animal parasite (rodents, cattle and sheep). Organisms from some (fish, fowl and reptiles) do not infect humans. • Infections in immunocompromised people can be serious, even fatal. • Identification - oocysts are 2 - 5 microns in diameter; do not stain with iodine; and are acid-fast.
The Protozoa Intestinal Coccidia Cryptosporidium parvum • Transmission - the endemic cycle is maintained via person-to-person, fecal-oral route transmission; a relatively common finding in “day-care” diarrhea; can be sexually transmitted; big potential for being waterborne due to significant resistance to disinfectants. • Pathology - most infections cause severe diarrhea. In the immunosuppressed patient, the condition is protracted and life threatening. There is no drug effective against this parasite.
The Protozoa Intestinal Coccidia Cyclospora cayetanensis • General - The first outbreak in the USA occurred in medical residents in 1980; a large multi-state outbreak occurred the summer of 1996. During this outbreak, Texas had more than 100 cases over a period of about six weeks, while no more than one case had been reported during any previous year. • Transmission - fecally contaminated food or water. The 1996 outbreak was associated with contaminated raspberries.
The Protozoa Intestinal Coccidia Cyclospora cayetanensis • Animal reservoirs - not known. Other Cyclospora species are known to infect a variety of animals, but C. cayetanensis is the name designated for the only one known to infect humans. • Pathology - diarrhea similar to that experienced with Cryptosporidium infections. • Identification - Oocysts are 10 microns in diameter, and are variably acid-fast.
The Protozoa Microsporidiumspp. • General - at this time, infections are thought to be limited to AIDS patients. • Transmission - person-to-person, via the fecal-oral route; can be sexually transmitted. • Identification - a very small organism, spores average 1.0 by 1.7 microns. They stain a reddish-pink color with Chromotrope stain. Some stained spores exhibit a dark staining “belt” across the middle of the organism.