Download

1 / 42
420 likes | 551 Views
web site: www.drsarma.in. Dr. R V S N Sarma., MD., MSc. (Canada), Consultant Physician & Chest Specialist Land line: 044 3760 9993 Mobile 91 9380521221 email: sarma.rvsn@gmail.com. THE Swine Flu BASIC INFORMATION. What Should be Our Approach?. Essential – Positive – Constructive Approach

E N D
web site: www.drsarma.in Dr. R V S N Sarma., MD., MSc. (Canada), Consultant Physician & Chest Specialist Land line: 044 3760 9993 Mobile 91 9380521221 email: sarma.rvsn@gmail.com THE Swine Flu BASIC INFORMATION
What Should be Our Approach? Essential – Positive – Constructive Approach • Adequate awareness in general public – adopting the preventive measures • Comprehensive knowledge for the healthcare providers • Appropriate planning and responsibility of all involved Unwarranted – Misleading – Dangerous – Negative • Fear, minute to minute monitoring of deaths, rumors • Media hype , Anxiety about infection and death by this flu • Panic, mania of mask use by one and all, and worry
Types of Human Flu (Influenza) • Influenza A • Common, More Severe, Several Sub-types • Epidemics, Pandemics, Mortality, High Mutagenicity • Influenza B • Less Severe, Less Frequent, No Sub types, Faithfully Human • Influenza C • Mild, Rare, No Sub types, Non fatal, Mild Illness in Children • Common Cold – Coryza Virus – It is not ‘Flu’
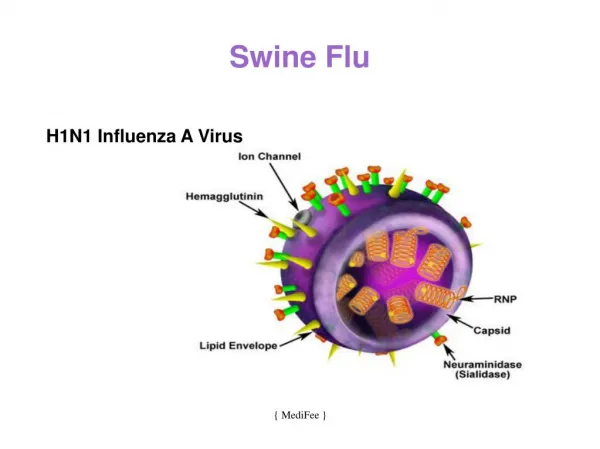
Influenza A Virus Types Neuraminidase (N) For Detachment Hemagglutinin (H) for Attachment • Orthomyxoviridae Family • Single stranded RNA virus • High mutagenicity, 8 proteins • H Ag types are 16 • N Ag types are 09 • So, 16 x 9 = 144 types possible • But only 3 types infect Humans • H1N1, H2N2 and H3N2 • Avian Flu Virus is H5N1 • ‘Swine Flu’ Virus H1N1 Misnomer • Present Pandemic – (H1N1)v
Natural History of H1N1v Mortality Rate = 15/1,00,000 = 0.015% 1,00,000 50,000 10,000 1,000 CFR = 15/10,000 or 0.15% 15
Symptoms of H1N1 Pandemic Flu • Very Similar to the Seasonal Flu and Not like Common Cold • Moderate to high fever • aches, muscle and joint pains • chills and fatigue • sore throat, head ache • cough • sneezing and running nose • shortness of breath, chest pain on breathing • diarrheas and vomiting (possible), loss of appetite
When to Suspect H1N1 ? Onset of acute febrile respiratory illness within 7 days of close contact with a person who has a confirmed case of H1N1 influenza A virus infection, or Onset of acute febrile respiratory illness within 7 days of travel to a community (within the United States or internationally) where one or more H1N1 influenza A cases have been confirmed, or Acute febrile respiratory illness in a person who resides in a community where at least one H1N1 influenza case has been confirmed.
Global Experience of the Pandemic Secondary attack rate in household contacts: 12 %. Overall proportion of hospitalizations: 8 %. Overall case fatality: 0.15 % or 1.5 per every 1000 cases Most cases (58 %) highest incidence in 5–24 years age group, Second highest incidence in children < 5 years Most hospitalizations (34 %) in 5–24 years age group, Highest age-specific hospitalization rate in children < 5 years Most deaths in 5–24 years age group The old are generally spared > 65
The Current H1N1 Virus • Cocktail mix of Porcine, Avian and Human Influenza A Virus • Direct • Fine droplets expelled during coughing and sneezing • Expectorated sputum and the dried secretion • Indirect • All items that have been in contact with a patient (Fomite) • Incubation Period (IP) • 3 to 7 days – from the day of symptoms – Median 2-3 days
High Risk Groups for H1N1 Diabetes Pregnancy Neuromuscular disorder Chronic cardio-vascular disease (excluding hypertension) Seizure disorder and other neurodegenerative disease Chronic renal disease stages III and IV Cancer and immuno suppression Obesity More deaths in people <18 years of age
Diagnostic Testing • rRT-PCR Swine Flu assay– reverse transcriptase real time PCR • Highly specific test, 24 to 48 hours, costly Rs. 4,000, detects viral multiplication, can identify the novel H1N1 correctly • Confirmatory test, sensitivity is also quite high 85%, Quantitative • RIDT (Rapid Influenza Diagnostic Test) – Not Recommended • point of care, 1 hour, less cost (Rs 700), card test, detects viral protein • Sensitivity low 10 to 70% - A negative result can’t exclude Influenza • Can not distinguish between Influenza B or A or A sub types • Specificity – 80% - can confirm Influenza infection – not the type • If positive – needs a confirmatory test to identify the type
Testing Facilities in Chennai • Government • King Institute, Guindy • Private • Bharat Scans, Royapettah • Hi-Tech Diagnostic Center, T. Nagar • Diagnostic Services, T.Nagar • Lister Metropolis • Sri Rama Chandra University
General Hygiene • Cover the mouth whenever you cough, then wash hands • Cover the nose every time you sneeze, then wash hands • Wipe with disposable tissue paper, throw into a garbage can covered with a lid and then wash hands • Do spit in a disposable tissue paper, throw into a garbage can covered with a lid and then wash hands • Hand hygiene, is essential and imperative, either washing with soap or by clean by rubbing alcohol based sanitizer. It must be done carefully and repeated as often as possible • Use of surgical mask and personal protection equipment (PPE)
General Treatment • Treatment is largely supportive • Bed rest; Patient should stay at home for 7 days • Increased fluid consumption; Cough suppressants and • Cough Etiquette, Hand washing • Antipyretics and analgesics (Paracetamol, NSAIDs) • Avoid close contact with sick person • May require intravenous hydration & supportive measures • Home Isolation; One designated person to take care
Categories of H1N1 (Govt. India) Category A: Common fever with cough and throat pain body pain and headache, diarrhea and vomiting. No need to test for A(H1N1). No Tamiflu. Under constant supervision for a three days. Cough etiquette. Category B: High fever and severe throat infection. Children < 5 years, pregnant women, Adults 65 + age and with complications of the kidneys, heart and lungs, diabetics and HIV. Give Tamiflu, but no test for A (H1N1). Home isolation. Category C: Same as Category B, but have breathlessness, chest pain, fainting spells, low blood pressure, blood in the phlegm, cyanosis, not taking feeds, altered sensorium. They need A (H1N1) test and be given Tamiflu and need hospitalization.
Oseltamivir (Tamiflu) It is a neuraminidase inhibitor (NAI), decreases the release of viruses from infected cells and, thus, viral spread. Must be administered within 48 hours of symptom onset Reduces the length of illness by an average of 1.5 to 2.5 days Duration of administration for treatment is 5 days Post-exposure prophylaxis to be initiated within 7 days of exposure and continued for at least 10 days Available as 30-mg, 45-mg, and 75-mg oral capsules and as a powder for suspension containing 12 mg/mL after reconstitution
Oseltamivir (Tamiflu) • Adult Dose • Acute illness: 75 mg PO bid for 5 days • Prophylaxis: 75 mg PO once a day for 10 days • Pediatric dose • Acute illness in children aged <1 year • <3 months: 12 mg PO bid for 5 d; 3-5 months: 20 mg PO bid for 5 d • 6-11 months: 25 mg PO bid for 5 d • Acute illness and age >1 year • <15 kg: 30 mg PO bid for 5 d; 15-23 kg: 45 mg PO bid for 5 d • 23-40 kg: 60 mg PO bid for 5 d; >40 kg: Administer as in adults
Zanamivir (Relenza) It is a neuraminidase inhibitor, decreases the release of viruses from infected cells and, thus, viral spread. Must be administered within 48 hours Adult Dose Treatment for acute illness: 10 mg inhaled orally bid for 5 days • Prophylaxis of household contact: 10 mg inhaled orally od for 10 d • Prophylaxis for community outbreak: 10 mg inhaled orally od for 28 d Pediatric Dose Treatment for acute illness • <7 years: Not established; >7 years: Administer as in adults Both are ‘Pregnancy Category C’ – Not a contraindication – prefer Zanamivir
Management of Severe Disease Most cases do not need Test, Tamiflu, Hospitalization Supportive treatment and home isolation will suffice Watch out for the high risk groups and Category B and C Early administration of Tamiflu if indicated; Reduces viremia Monitor O2 saturation and maintain 90-92% saturation - O2 Rx. Antibiotics for secondary bacterial pneumonia – as per CAP MRSA; Ventilator support in severely ill – VAP; Vasopressors No role for corticosteroids except in shock; Risk is increased ARDS – Lung protective mechanical ventilation
Executive Summary Airborne transmission – No unusual routes – Food no risk Cumulative clinical attack rate – 20 to 30% Over 90% of the illness is mild and self limiting Highest affected will be children and young adults Adults > 60 years seem to be least affected High risk groups discussed must be watched for fatality Hospitalization rates will be 1 to 2% of clinical cases The term ‘swine flu’ is inaccurate & confusing– AH1N1v 2009
Executive Summary • Case Fatality Rate will be around 0.1 to 0.2% (1-2 per 1000) • Fatality will be more in children and very old and high risk • Hospitalizations are for high risk groups, people < 5, > 60 y • H1N1v is sensitive to Oseltamivir and Zanamivir – NAIs • Seasonal flu vaccine is ineffective; Vaccine in October • The virus can mutate at any time – Second wave aggressive • International co-operation and sharing of experience • All these rates & ratios are biased upwards – inapparent inf.
What We Know? This Flu is like any other ARI Cover your cough and sneeze Frequent hand washing Hand – face distancing Social distancing Fomite transmission – cell phones Home isolation; Discuss the need for Test and Tamiflu Only a small proportion need hospitalization Flu death is very rare; No need to panic
What Should We do? Remember is similar in most respects like any other ARI Suspect the pandemic flu – particularly if temp is > 100 Look for signs of serious illness – SOB, chest pain, blood etc Look for high risk profile, Be watchful about young kids Categorize the patient as A, B or C and note the stage Take appropriate action as per the category Segregate patients at first contact in the waiting room Give priority to those with ARI and reduce contact time Protect yourself with mask while examining a suspect case
Top Resources Consulted http://www.emedicinehealth.com/swine_flu/article_em.htm#history http://www.who.int/csr/disease/swineflu/en/index.html http://www.who.int/csr/disease/avian_influenza/phase/en/ Journal of Applied Microbiology 91 (4): 572–579, 2001 http://knol.google.com/k/salim-djelouat/swine-flu-pandemic-review http://emedicine.medscape.com/article/1673658-overview http://www.cdc.gov/h1n1flu/general_info.htm http://www.cdc.gov/h1n1flu/ http://www.cdc.gov/h1n1flu/surveillanceqa.htm http://www.cdc.gov/h1n1flu/masks.htm
Top Resources Consulted… contd http://www.cdc.gov/h1n1flu/guidance/rapid_testing.htm http://www.cdc.gov/h1n1flu/recommendations.htm http://www.ecdc.europa.eu/en/Pages/home.aspx http://www.ecdc.europa.eu/en/healthtopics/PublishingImages/World_Map http://sis.nlm.nih.gov/enviro/swineflu.html#a3 New England Journal of Medicine: H1N1 Influenza Center http://www.lancet.com/H1N1-flu http://h1n1.nejm.org/?ssource=rthome http://pandemicflu.bmj.com/ H1N1 Clinical Medical References & Guidelines @ MDConsult.com