Download
1 / 19
210 likes | 632 Views
Ultrafiltration Control using Hematocrit Monitoring. 2013 ANNA North Carolina Statewide Symposium and the Southeastern Kidney Council NC Annual Meeting “Unique Challenges for the Nephrology Professional” Kimberly F. Clarkson, MSN, RN, CNN May 22, 2013. Objectives.

E N D
Ultrafiltration Control using Hematocrit Monitoring 2013 ANNA North Carolina Statewide Symposium and the Southeastern Kidney Council NC Annual Meeting “Unique Challenges for the Nephrology Professional” Kimberly F. Clarkson, MSN, RN, CNN May 22, 2013
Objectives • Describe blood volume monitoring • Identify trend and graph development during hemodialysis • Evaluate nursing assessment considerations to decrease intradialytic mortality
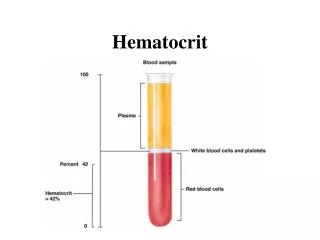
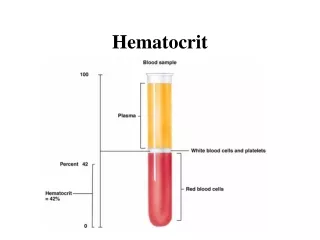
Relative Blood Volume Monitoring • Measures hematocrit in arterial blood • Crit-Line® Technology • Optical transmission detecting blood volume changes • Blood volume change – surrogate marker for vascular refilling • Increase in hematocrit relative to decrease in fluid removal • Interface display of changes • Affords a “window” into intravascular space Davenport, 2009
Prevention through Optical Technology • Components • Blood chamber, sensor clip, monitor • Non-invasive monitoring • Blood volume change percent • Hematocrit • Graphic display • Based on Guyton curve
Guyton’s Curve • Dr. Guyton (September 8, 1919 -April 3, 2003) • Physiologist; primarily circulatory system • Cardiac output related to peripheral circulation • Demonstrated oxygen demand regulated cardiac output • Overturned previous conventional wisdom • Heart itself does not control output • Developed graphic representation • Fundamental base in medical school • Guyton Curve Hall, 2003
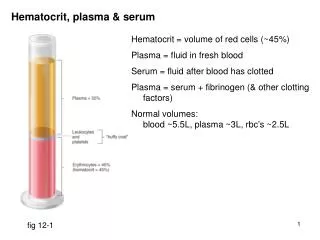
Fluid Volume Distribution • Volume distribution; 70 kilogram male example • Intracellular • Approximately 23 L • Extracellular • Approximately 17 L • Intravascular • Approximately 5 L; cannot accommodate > 7 L
8 A Edema 7 6 B Low O2 Meds UFR Na+ Temp Posture 8 5 Normal Shift Due to: 7 4 Blood Volume (liters) C 3 6 Hypovolemia 2 Death 5 1 0 4 Adapted from Guyton, AC: Textbook of Medical Physiology, 1991, pg.324 3 Normal 40 0 5 10 15 20 25 30 35 2 Extracellular Fluid Volume (liters) Blood Volume (liters) 1 0 0 40 5 10 15 20 25 30 35 Death Adapted from Guyton, AC: Textbook of Medical Physiology, 1991, pg.324 Extracellular Fluid Volume (liters) Guyton’s Curve Applied
Optical Data Transformed – Graphic Image The Crit-Line®monitor provides objective data and visual display of: • Relative Plasma Volume slope as an indicator of volume status • Degree of Relative Blood Volume Slope • Remember Guyton Curve • Intradialytic plasma refill ability or inability • In comparison to ultrafiltration • Intradialytic plasma refill with minimal ultrafiltration
35 33 Hct 31 29 RCV 27 X 100 Hct = 0 BV -5 %BV (Loss) -10 -15 -20 0 1 2 3 4 The Inverse Relationship
Profile A • Ultrafiltration and plasma refill • Equal, or positive slope or slope less than -3% • Special considerations may apply Hypertension, 2010
Note: UF Removed Note: BV∆%
-8.6% ÷ 3.3 hour = -2.6% per hour = Profile A
Profile B • Ultrafiltration rate exceeds plasma refill rate • Studies range from -1.33% per hour to -8% per hour • Not to exceed -16% at end of 3 to 4 hour treatment Agarwal, 2010
-12.8% ÷ 3 hours = - 4.3%/hour = Profile B
Profile C • Patient “crash” • Patient experiences symptom • Blood volume change • Exceeds -8% per hour, or • Exceeds -16% at end of 3 to 4 hour dialysis session Rodriguez et. al,2005 Brewer & Goldstein, 2004
-20.9 ÷ 2 = -10.4 = Profile C
Prevent Treatment Complications E – Electrolytes V – Volume removed–ultrafiltration A – Anemia/albumin/allergies L – Lying back, feet on floor – position U – Urinary output A – Anti-hypertensives or other meds T – Temperature I – Ideal dry weight O – Oxygenation of tissues N – Nurse responsibility
Summary • Hematocrit monitoring affords a proactive approach to • Achieve ideal dry weight • Prevent intradialytic complications • Prevent hospitalizations • Affords validation of nursing interventions • Real time measurement • Data provision – graphical representation • Individualized patient