Download
1 / 59
590 likes | 766 Views
Genitourinary Medicine. For GPs November 2007. Agenda. Recent changes How to take the necessary swabs Brief overview STI’s What can be done in General Practice Cases. New diagnosis of selected STIs in GUM clinics, England, Wales and Northern Ireland.

E N D
Genitourinary Medicine For GPs November 2007
Agenda • Recent changes • How to take the necessary swabs • Brief overview STI’s • What can be done in General Practice • Cases
New diagnosis of selected STIs in GUM clinics, England, Wales and Northern Ireland
Chlamydia • Common (3-5% sexually active females attending UK General Practice) • Complications cost at least £50million annually in the UK
CLINICAL FEATURES(chlamydia) • 80% Females asymptomatic • PCB/IMB, abdo pain, discharge,cervicitis • 50% males asymptomatic • Urethral discharge, dysuria • RISK FACTORS FOR INFECTION • COMPLICATIONS
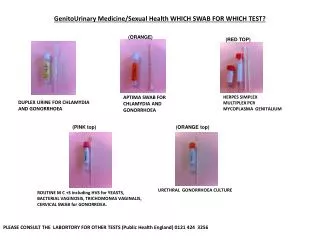
DIAGNOSIS(chlamydia) • Women endocervical swab gives best specimen • Urethral swabs will identify additional 10-20% • Men urethral swab (painful!) • ELISA vs PCR • Urine testing
WHAT CAN I DO IN PRACTICE?(chlamydia) • 1. POSITIVE RESULT BACK • Treat patient • Contacts need treatment • Advised no SI until both partners treated • Can refer to clinic for full tests • Guidelines say only retest if symtomatic/possibility of reinfection at 3 weeks
TREATMENT(chlamydia) • Doxycycline 100mg bd 7 days • Azithromycin 1g orally as single dose • Erythromycin 500mg qds 10 days (pregnancy) • Ofloxacin 200mg bd 7 days
GONORRHOEA ‘THE CLAP’ • CLINICAL FEATURES • Women 50% asymptomatic • Vaginal discharge, abdo pain, dysuria • Rarely causes IMB/menorrhagia • Pharyngeal infection asymptomatic >90% • Men 80% discharge, 50% dysuria • Rectal symptoms • Signs
DIAGNOSIS(gonorrhoea) • Laboratory culture • Microscopy • NB: Specimen collection sites
WHAT CAN I DO IN GENERAL PRACTICE? • Refer any patients with confirmed GC on swabs to GUM • Refer any acute urethral discharge • Refer contacts of GC to GUM for treatment and ix • Refer females with lower abdominal pain
TREATMENT(gonorrhoea) • Cefixime 400mg oral as single dose • Ciprofloxacin 500mg stat • Spectinimycin 2g IM single dose • Ceftriaxone 250mg IM ( pregnancy)
FOLLOW UP • 2 Weeks TOC in clinic • Pregnant women, symptomatic patients • Check contacts have been treated/tested • Be aware of possible co-infection with chlamydia
NSU • Male urethritis in the absence of gonorrhoea • Mucopurulent cervicitis equivalent condition in female • 30-50% due to chlamydia • 20% due to mycoplasma genitalium
Clinical Features • Urethral discharge, dysuria, irritation (M) • Vaginal discharge (usually asymptomatic) • DIAGNOSIS • Microscopy • Swabs, check for chlamydia
TREATMENT • Doxycycline 100mg bd for 7 days • Azithromycin 1g as a single dose • Treat contacts
GENITAL HERPES • HSV 1/ 2 • Common • Incubation period 1-2 weeks • Asymptomatic shedding • Chronic condition • Psychological aspects
CLINICAL FEATURES • Painful ulceration, dysuria, vaginal or urethral discharge • May be systemically unwell • Blistering/ulceration external genitalia • Inguinal lymphadenopathy • COMPLICATIONS: urinary retention, aseptic meningitis
DIAGNOSIS • Isolation of HSV from genital lesions • Often a clinical diagnosis • Serology, not routinely done
WHAT CAN I DO IN GENERAL PRACTICE? • Take a viral culture swab • General advice: saline bathing, analgesia, topical anaesthetic, petroleum jelly • Start oral antiviral drugs (within 5 days) • Aciclovir 200mg five times a day for 5 days • Psychological support • Arrange F/U GUM 3-4 weeks for full tests
GENITAL WARTS • Human papillomavirus (HPV) • >90 genotypes • Nearly always sexually transmitted • Common • Difficult and time consuming to treat • Certain types associated with cervical dysplasia • Benign epithelial skin tumours
DIAGNOSIS • Most cases naked eye examination • Colposcope helps • May need biopsy if dx uncertain
What can I do in General Practice? • Refer GUM for full assessment • Will not need urgent assessment if no other symptoms present • You can give warticon lotion/cream if confident of dx
TREATMENT IN CLINIC • All treatments have significant failure and relapse rates • Podophyllin, trichloroacetic acid, cryotherapy • Home treatments are warticon and aldara (imiquimod) • (HPV vaccine)
TRICHOMONAS • Flagellated protozoan • Almost exclusively sexually transmitted • Female symptoms: discharge, itching, odour, abdo pain. 10-50% are asymptomatic • Male symptoms: urethral discharge/ dysuria. 10-50% asymptomatic
Diagnosis/Management(trichomonas) • HVS • Direct observation wet smear • More difficult to culture in men • Treat sexual partners simultaneously • Metronidazole 400mg bd 5-7 days or 2g stat • Refer GUM for full tests
Bacterial Vaginosis • The commonest cause of vaginal discharge in women childbearing age • Replacement of lactobacilli and raised Ph • Not regarded as sexually transmitted
SYMPTOMS/SIGNS • 50% women asymptomatic • ‘fishy’ vaginal discharge • Thin/white discharge • In pregnancy BV is associated with late miscarriage, preterm birth, preterm premature rupture of membranes, post partum endometritis
Diagnosis • HVS • Gram stain
What shall I do in general practice? • Treatment is indicated for symptomatic and pregnant women • You do not have to treat asymptomatic women but can offer treatment • General advice re vaginal douching, use of soap etc • Treatment: metronidazole 400mg bd for 5-7 days or 2g stat • Clindamycin cream 2% daily 7 days, metronidazole gel 0.75% daily 5 days
Vulvovaginal Candidiasis • Candida. albicans approx 90%, candida.glabrata approx 10% • 10-20% women of childbearing age may harbour candida species in the absence of symptoms. They do not require rx • Symptoms/signs • Beware the woman with ‘recurrent thrush’ • Do a HVS