Download
1 / 26
760 likes | 2.55k Views
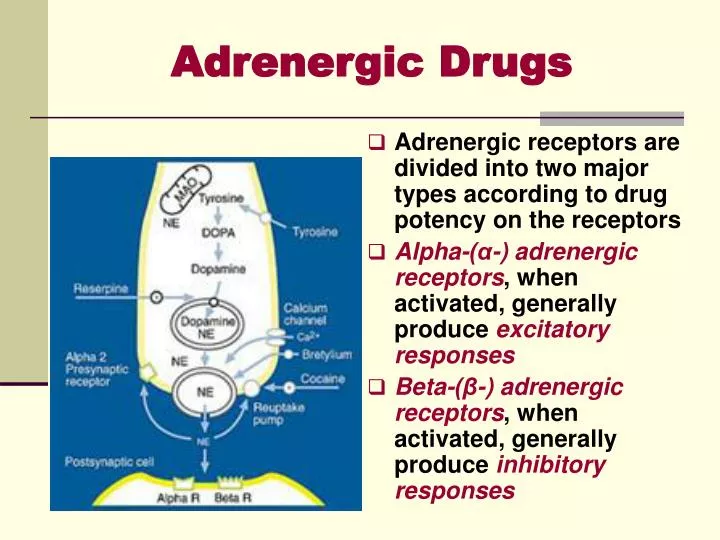
Adrenergic receptors are divided into two major types according to drug potency on the receptors Alpha-(α-) adrenergic receptors , when activated, generally produce excitatory responses Beta-(β-) adrenergic receptors , when activated, generally produce inhibitory responses. Adrenergic Drugs.

E N D
Adrenergic receptors are divided into two major types according to drug potency on the receptors Alpha-(α-) adrenergic receptors, when activated, generally produce excitatory responses Beta-(β-) adrenergic receptors, when activated, generally produce inhibitory responses Adrenergic Drugs
Direct-acting Adrenergic AgonistsA. Catecholamines • Catecholamines, adrenergic neurotransmitters; L-norepinephrine (NE), L-epinephrine (E), & L-dopamine (DA) in addition to the synthetic analog isoproterenol • They have the following characteristics: • High potency • Rapid enzymatic inactivation by MAO & COMT as well as neuronal & non-neuronal uptake • Therefore they have short duration when given parenterally and are inactive orally • Poor ability to pass the CNS
Direct-acting Adrenergic AgonistsB. Non-catecholamines • Non-catecholaminesare adrenergic agonists lacking the catechol hydroxyl groups • Therefore they are of longer duration, can be given orally and they are not inactivated by COMT • They include agents like phenylephrine, ephedrine and amphetamine
General Mode of Action of Adrenergic Agonists • Direct-acting agonists that act directly by binding to the adrenergic receptors, include NE, E, DA, phenylephrine & isoproterenol • Indirect-acting agonists that cause the release of NE from intra-neuronal storage vesicles by the virtue of being taken up by the pre-synaptic adrenergic neurons • They include agents like amphetamine and tyramine • Mixed-action agonists, ephedrine
Pharmacological ActionsA. Nonselective Direct-acting Adrenergic Agonists 1- Cardiac Effects • Increased force of contraction(positive inotropic effect) • Enhanced automaticity of latent pacemaker cells that may lead to arrhythmias • Acceleration of impulse conduction velocity(conductivity) between the atria and ventricles via shortening of the refractory period of the A-V node • Increased stroke volume and cardiac output but with accompanied rise in oxygen consumption • The heart efficiency (performance) is decreased in terms of lower cardiac work in relation to oxygen consumed • Reflex bradycardia, NE, and E but in high doses
2) Vascular Smooth Muscle Effects • NE constricts all blood vessels except the coronary vascular bed (α>β2) • E has mixed effects according to the vascular bed (β2> α), dilation in skeletal muscles, liver & coronaries • Isoprenaline has purely vasodilatotory effects (β2>>> α)
Effects of I.V. infusion of Epinephrine, Norepinephrine & Isoprenaline in Humans
3- Effects on Gastrointestinal Tract Relaxation of GIT smooth muscle through • Inhibition of the release of ACh from cholinergic neurons via activation of α2-adrenoceptors on cholinergic nerve terminals • Stimulation of β2-receptors, activates adenyl cyclase-c.AMP- PKA cascade leading phophorylating inactivation of myosin-light chain kinase enzyme • Stimulation of α1-adrenoceptors causes increased potassium channel activity resulting in increased K+ conductance & hyperpolarization
4- Effects on Respiratory System • β2-Adrenoceptors stimulation leads to relaxation (inhibition) of bronchiolar smooth muscle and bronchodilation, and hence lowering airway resistance (Asthma) • Inhibition of antigen-mediated production of inflammatory mediators of asthma via β2-adrenoceptorsstimulation (Asthma) • α1-Adrenoceptors activation results in vasoconstriction of the upper respiratory tract mucous membranes and hence lowering congestion (Nasal decogestant)
5- Effects on the Uterus • They are dependent on the uterine status • Norepinephrine increases the rate of contraction of pregnant human uterus • Epinephrine inhibits uterine tone and contractions during the last month of pregnancy as well as at parturition • This observation is the basis for the use of β2-adrenoceptors agonists to delay premature labor
6- Effects on the Eye • Stimulation of α1-adrenoceptors on the radial smooth muscle of the iris leads to pupil dilation (mydriasis), theoretically result in blocking of drainage of aqueous humor and increase of IOP • α1-adrenoceptors stimulation results in vasoconstriction that in turn causes inhibition of the formation of aqueous humor & lowering of IOP • This latter effect usually predominates
7- Metabolic Effects • Lipolysisis stimulated leading to increased breakage of triglcerides into free fatty acids and glycerol through activation of lipase enzymatic activity (β1/ β3-adrenergic receptor stimulation-increased c.AMP-PKA activation -phosphoryaltion of lipase) • Hepatic & Skeletal Muscle Glycogenolysisare stimulated resulting in hyperglycemia & increased plasma glucose & lactic acid (β2-adrenergic receptor stimulation with subsequent activation of adenyl cyclase-c.AMP-PKA cascade-Activated PKA phosphorylates phosphorylase kinase - activates phosphorylase) • Calorigenic action where oxygen consumption is increased in response to catecholamines mainly due to increased oxidisable substrate from increased lipolysis in adipose tissues
Selective α1-Adrenergic Agonists Phenylephrine & methoxamine • elevated systolic & diastolic BP • increased total peripheral resistance • barororeceptor mediated reflex decrease in heart rate via enhancement of vagal activity • They are less potent but longer acting than norepinephrine, being non susceptible to metabolism with COMT
Therapeutic Uses of α1-Adrenergic Agonists • Local nasal decongestantto produce vasoconstriction of nasal mucosal vasculature • Treatment of supraventricular tachycardia arising in AV node and atria • They elevate blood pressure & stimulate vagal activity via baroreceptor-mediated reflex action • To overcome hypotension induced by some general anesthetic agent
α2 -Adrenergic Agonists • Clonidine & α-methyldopa activate α2-Adrenergic receptorsin the lower brain stem (nucleus of tractus solitaries) leading to decreased central outflow of the sympathetic nervous system • Oral intake produces a prolonged hypotensive response (Treatment of Hypertension) • IV injection raises BP by direct stimulation of postsynaptic α1- & α2-Adrenergicreceptors • In addition, α-methyldopa is taken up by adrenergic neurons and synthesized into α-methylnorepinephrine which is a false adrenergic transmitter
β1-Adrenergic Agonists • Dobutamineis a synthetic dopamine analog. It is a selective β1-adrenergic agonist. On the heart, it produces a more pronounced positive inotropic effect than its chronotropic effect when compared to dopamine. There is no defined reason for such differential action • It produces renal and mesenteric vasodilation (D1-receptors) similar to dopamine • Therapeutic use of dobutamine is based on its ability to increase cardiac output via the positive inotropy with little effect on heart rate and myocardial oxygen consumption • Hence, it is used in cardiogenic shock and decompensated heart failure
β2 adrenergic receptor agonists • Terbutaline, albuterol (salbutamol), & ritodrineare selectiveβ2 adrenergic receptor agonists with little effect on β1 cardiac receptors • Hence, they have the advantage of producing bronchodilation without cardiac stimulation • They produce uterine relaxation • They are given orally, IV or by inhalation and long duration of action and possess no CNS stimulation • Therapeutic uses of β2 adrenergic receptor agonists • Treatment of bronchial asthma and bronchospasm associated with bronchitis and emphysema • Delay delivery in premature labor and in threatened abortion; ritodrine is frequently used for this purpose
Indirect- & Mixed-Acting Adrenergic Receptor Agonists • Ephedrine • Chemically related to EP and stimulates release of NE • It is not a substrate forCOMT or MAO & hence has long duration of action • It activates β2 as well as α- and β1-aderenergic receptors • It is used to treat mild cases of asthma • It crosses BBB giving rise to CNS stimulant action • It is now replaced by more selective β2 agonists • Tyramine in cheese, fermented sausage & wines • It enters synaptic vesicle and causes displacement & release of NE & normally degraded by MAO • MAO inhibitors in conjunction with tyramine-containing foods may lead to rapid release of NE & severe hypertension
Indirect- & Mixed-Acting Adrenergic Receptor Agonists • Pseudoephedrine & Phenylpropanolamine • They stimulate the release of NE • They are used as over-the-counter (OTC) nasal decongestants for symptomatic relief of hay fever and rhinitis • Pseudoephedrine has little β2 agonist activity, limited CNS stimulation • Phenylpropanolamine also used to relieve upper respiratory conditions associated with common cold
Clinical uses of α- & β-Adrenergic Agonists • Nasal decongestant: Vasoconstriction in nasal mucous membranes by α1-agonists like phenylephrine, pseudoephedrine & xylometazoline • Treatment of hypotension • Selectiveα1-agonistslike phenylephrine, methoxamine & mephentermine are administered parenteraly to elevate blood pressure in hypotension accompanying spinal anesthesia. They cause prompt vasoconstriction increasing total peripheral resistance and hence raising diastolic and systolic pressures • In hypovolemic shock use of α1-agonistshas the potential to cause further impairment of microcirculation already affected by high level of catecholamine release
Clinical uses of α- & β-Adrenergic Agonists • Cardiogenic shock (MI), NE, dobutamine or DA • NE is given by ONLY IV infusion at doses that raise BP, and increase cardiac contractility without serious vasoconstriction • Dopamine is advantageous in producing splanchnic and renal vasodilation (D receptors), increasing glomerular filtration and urine production • Dobutamine is more or less similar to dopamine being more selective on cardiac β1-adrenergic receptors
Clinical uses of α- & β-Adrenergic Agonists • Anaphylactic Shock: Epinephrine is of choice given by SC route to reverse the histamine-induced broncho-constriction & hypotension • Opthalmic Uses: • Mydriatics: phenylephrine & ephedrine may be used for eye examination • Glaucoma: phenylephrine or epinephrine may be used locally to decrease IOP
Clinical uses of α- & β-Adrenergic Agonists • 5- Respiratory uses: • Treatment of asthma using theselective β2 adrenergic receptor agonists including terbutaline, albuterol and orciprenaline by oral route or by inhalation. They have fewer cardiovascular stimulant effects • Relieve of congestion of upper respiratory tract in hey fever and rhinitis. For this purpose, α1 agonists such as phenylephrine, pseudoephedrine & phenylpropanolamine can be used orally to produce vasoconstriction of mucous membrane vasculature
Clinical uses of α- & β-Adrenergic Agonists • As Vasoconstrictors with Local Anesthetics: Epinephrine and phenylephrine may be used to produce localized vasoconstriction which inhibits systemic absorption and lower bleeding • Epistaxis; Epinephrine (1:100,000 dilution) or -agonists may be used to stop bleeding from nasal mucosa • Cardiac arrest; Epinephrine or isoprenaline may be used by IV roué or by intra-cardiac injection • They may be used in complete heart block