Download
1 / 24
240 likes | 456 Views
On Surrogate Endpoints in HIV Vaccine Efficacy Trials . FDA/Industry Statistics Workshop, Sept 18-19, 2003 “Statistics: From Theory to Regulatory Acceptance”. Steven Self, Peter Gilbert, Michael Hudgens FHCRC/UW. Outline. HIV Vaccine Trials: Current Status

E N D
On Surrogate Endpoints in HIV Vaccine Efficacy Trials FDA/Industry Statistics Workshop, Sept 18-19, 2003 “Statistics: From Theory to Regulatory Acceptance” Steven Self, Peter Gilbert, Michael Hudgens FHCRC/UW
Outline • HIV Vaccine Trials: Current Status • Clinical Endpoints in Vaccine Trials • Endpoints in HIV Vaccine Trials • A Simulation Approach • Goal • Approach • Example • Conclusions/Discussion
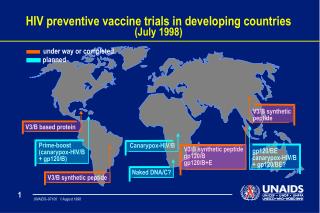
HIV Vaccine Trials: Current Activity • Phase I and II trials (ongoing) • 27 trials involving ~1,800 participants • 16 different vaccine candidates • 10 sponsors • Phase III trials • 1 completed • 1 to be completed in Q4 ’03 • 1 planned to start in ’04 • HVTN trials (Ph I, II) starting by Q3 ’04 • 9 different vaccine candidates • 1,453 participants
HIV Vaccine Trials: Current Results • Immune Responses • Measurable cellular response in ~50% • No broadly neutralizing Ab in sera, mucosa • Non-human Primate Trials • Amelioration of disease course but no protection from infection upon challenge • Body of NHP literature difficult to assess • Efficacy • No overall efficacy in 1 completed efficacy trial
HIV Vaccine Trials: Summary • Immune correlate of protection unknown • Many candidate vaccines but full range of desired immune responses poorly covered • Multiple efficacy trials will be required* • Plan for long-term, iterative development program* * Klausner et. al. (2003) Science
Classical Measure of Vaccine Efficacy VE = % reduction in population incidence or morbidity/mortality rate
Classical Endpoint for Vaccine Efficacy • Clinically significant morbidity and mortality • Pathogen specificity • Standard of care • For treatable infections: • Prevent/delay constellation of signs/symptoms sufficient to trigger treatment initiation (save cost/toxicity assoc with treatment) • Interact w/ treatment to improve risk/benefit profile of vaccine/tmt vs tmt alone
Measures of Vaccine Efficacy* VE = % reduction in population incidence or morbidity/mortality rate VES = % reduction in population infection rate VEP = % reduction in rate of morbidity/mortality VEI = % reduction in rate of 2o transmission * Halloran, Longini, Struchiner
VE: % Reduction in Transition Intensities VE VES VEP Uninfected/ Seronegative Infected/ Seropositive Morbidity/ Mortality VEI 2o Transmission
Endpoints in HIV Vaccine Efficacy Trials • “Infection” Endpoint (A biomarker-based surrogate) • Operationally: presence of Ab and detectable HIV RNA • Aligned with one primary objective of HIV vaccine • Acceptable by all • However captures only one aspect of potential vaccine effects on clinical outcomes
Endpoints in HIV Vaccine Efficacy Trials “Post-infection” Endpoints: Some Issues • Long-term FU required for morbidity/mortality endpoints esp with ARV treatment • Complicated dynamical process likely dominated by treatment effects • Uncertainty of optimal treatment initiation triggers • Variability in treatment initiation • Analytics • Key biomarker trajectories “dependently censored” by treatment initiation • Conditional vs unconditional analyses • Combination of analyses
Post-Infection Endpoints: Current Approach • Provide treatment within trial • standardized treatment initiation guidelines (e.g. DHHS, UNAIDS) • standardized treatment monitoring/management • Develop complementary array of endpoints to cover key aspects of post-infection outcomes • Early Endpoints - pre-ART • Mid-term Endpoints - peri-ART • Long-term Endpoints - post-ART • “Reasonable conservatism” for interpretation of vaccine effects on surrogates
HIV Vaccine Efficacy Trial Endpoints Long-term Endpoints: - vaccine/tmt effects - CD4 - Morbidity/Mortality Short-term Endpoints: - Pre-ART VL Uninfected/ Seronegative Infected/ Seropositive Morbidity/ Mortality Treatment Initiation Mid-term Endpoints: - Composite (VL, tmt init) - Biomarker trajectories (VL, CD4) Infection
A Composite Endpoint • Definition: • First event of ART initiation or virologic failure • (VL > X cps/ml) • Composite endpoint directly tied to clinical events • virologic failure places a subject at risk for progression/transmission • starting ART exposes a subject to drug toxicities, resistance, loss of future drug options • Assess with standard statistical methods (Kaplan-Meier, Cox regression)
A Composite Endpoint • Surrogate vaccine efficacy parameter: • VEVLC(T;X) = percent reduction (vaccine vs. placebo) in the risk of the composite endpoint by T months post infection diagnosis • X calibrates themagnitude of virologic control • (e.g., X = 1,500 copies/ml) • T calibrates the durability of virologic control • (e.g., use T 18 months)
A Numerical Study*: Goal • Provide an approach to facilitate the discussion of how to use surrogate endpoints • specific to trial design • specific to particular surrogate endpoints • accommodate statistical uncertainties • accommodate model uncertainties with desired degree of conservatism * Gilbert et al (2003) JID
A Numerical Study: Approach • adopt empirically-based joint model of biomarker process and clinical outcomes as “true” prediction model* • modify model to incorporate degrees of “reasonable conservatism” • proportion vaccine effect explained** (attenuate log RR relating surrogate to clinical outcome by f percent ) • selection bias for conditional analyses*** (attenuate observed vaccine effect on surrogate outcome) • RCT simulation to identify minimum observed effects on specific surrogate endpoints that would generate 95% prediction intervals for VE parameters exceeding 40%, say * Albert et al (1998) Stat in Med ** Freedman et al (1992) Stat in Med *** Hudgens et al (2003) Stat in Med; Gilbert et al (2003) Biometrics
Numerical Study: An Example • Question: • What inference on VEVLC(18;X) “reasonably” predicts a clinically significant VEP? • Numerical study based on the following predictions: • from the MACS*: Predicted(VEP) = VEVLC(18;X) • for X 5,000-10,000 cps/ml • * Albert et al (1998) Stat in Med
Hypothetical Efficacy Trial The numerical study is based on the following hypothetical trial:
Prediction of VEP • A lower 95% confidence bound for VEVLC(18;X) > 50% predicts VEP > 40% with f = 0.375
Summary/Conclusions • Use of surrogate endpoints in HIV vaccine efficacy trials is question of how not whether • A framework is proposed to help interpret observed effects on surrogate endpoints that is • specific to particular trial designs/endpoints • captures relevant aspects of magnitude and durability of effect on surrogates • uses available empirical information relating biomarkers to clinical outcomes • is tunable with respect to degree of conservatism w/r/t use of empirical information • flexible to evolve with development program
Summary/Conclusions • HIV vaccines showing strong and durable effects on post-infection endpoints should be licensed • use of standardized ART guidelines important • use simulation studies to assist in building agreement about defining “sufficiently strong” and “sufficiently durable” • design trials to detect significant levels of either VES or VEVLC(T;X) • use supporting data on other endpoints • Long-term follow-up needed • for assessing VE and VEP directly • better understanding of surrogate endpoints