Download
1 / 20
200 likes | 315 Views
Using SNOMED CT in ABF initiatives. Australian e health research centre . Dr David Hansen | CEO . May 2013. Operational context NSW Health, FirstNet and other adopters SNOMED CT & Emergency Department Reference Set (EDRS) Activity Based Funding (MDBs and URGs) Wider context PCEHR

E N D
Using SNOMED CT in ABF initiatives Australian e health research centre Dr David Hansen| CEO May 2013
Operational context • NSW Health, FirstNet and other adopters • SNOMED CT & Emergency Department Reference Set (EDRS) • Activity Based Funding (MDBs and URGs) • Wider context • PCEHR • E health • Health reform agenda
A Reminder: Why are we doing Terminology? It’s about Data Quality and Interoperability PRIMARY SECONDARY TERTIARY Clinical users Care delivery Interoperability Decision Support Public Health Health Service Management Resource Allocation Funding Re-use (within) Re-purpose (between) Re-purpose (between) Clinical terms Classification categories Funding groups
Data management for ABF in ED v1.3 specifications
Mapping: inefficient, inaccurate Changes ?
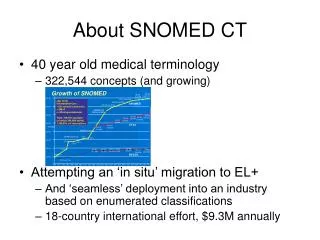
EDRS content (as provided) Concepts = 5 341 Paths = 28 857
EDRS Paths and maps (detail, single concept example) OPEN WOUND 125643001 = T14.1
No ICD-10-AM maps Disconnected concepts EDRS (detail) NOT a properly formed, functional RefSet
Missing terms? Terms that are important for clinical care not “in scope” of EDRS
Versions synchronised? EDRS treated as static, SNOMED versioning ignored Maps from SNOMED to ICD 10 AM invalidated, out-dated or missing
Material effect IHPA, URG grouper, v1.3
How to use SNOMED CT in ABF • Proposal • Build a clinically relevant EDRS • Don’t rely on maps • Aggregate SNOMED CT directly to MDB • Swap out the library files
Development experiment • Build a better EDRS • Find SNOMED CT concept that ‘matches’ MDB • Inherit all descendants (subsumption) • Manage membership, aggregation and versioning • Use proper tooling (Snorocket, Snapper, Ontoserver) • Transitive closure & transitive closure reduction algorithms • Directed Acyclic Graph traversal algorithms, rule based • Proof of concept • Trial with two MDBs • 3L: Gynaecological Illness • 4: Psychiatric Illness
Tertiary MDB 3L Gynaecological Illness Secondary Primary Concepts = 1 568 Paths = 6 492
MDB 4 Psychiatric Illness Concepts = 1 536 Paths = 3 936
How it would work Library file ICD to MDB Library file SNOMED CT – EDRS to MDB OR OR
Getting there from here • New approach to terminology management & tools • New EDRS required • Adequate and accurate specifications • Sufficient documentation, content and technical • Clinical user acceptance testing • Data testing, with queries and analytic approaches • Published test results
Key messages • Secondary and tertiary data can be driven by clinical data • Mapping not sustainable • Version management essential • Align with and exploit e-health initiatives
Thank you Dr David HansenCEO t +61 7 3253 3610 eDavid.Hansen@csiro.au whttp://aehrc.com • Australian e health research centre