Download

1 / 28
661 likes | 2.44k Views
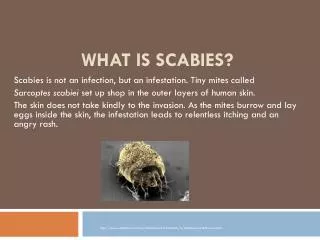
SCABIES. Causative organism: scabies mite sarcoptes scabei var hominis . an obligate human parasite Animal scabies mites may result in transient symptoms in humans, but they are not a cause of persistent infestations.

E N D
Causative organism: scabies mite sarcoptesscabeivarhominis. an obligate human parasite • Animal scabies mites may result in transient symptoms in humans, but they are not a cause of persistent infestations. • Transmission is via direct and prolonged contact with an infected individual.
Mites can survive up to 3 days away from human skin, so fomites such as infested bedding or clothing are an alternate but infrequent source of transmission. • The entire life cycle of the mite lasts 30 days and is spent within the human epidermis. • After copulation, the male mite dies and the female mite burrows into the superficial skin layers and lays a total of 60-90 eggs.
The ova require 10 days to progress through larval and nymph stages to become mature adult mites. Less than 10% of the eggs laid result in mature mites. • Mites move through the top layers of skin by secreting proteases that degrade the stratum corneum. • They feed on dissolved tissue but do not ingest blood. Scybala (feces) are left behind as they travel through the epidermis.
Upon initial infestation, a delayed type IV hypersensitivity reaction to the mites, eggs, or scybala develops over the ensuing 4-6 weeks • Previously sensitized individuals can develop symptoms within hours of reexposure. • Scabies occur primarily in institutional settings such as prisons and long-term care facilities such as nursing homes and hospitals. • Natural disasters, war, and poverty lead to overcrowding and increased rates of transmission.
Complications • Complications of scabies are rare and generally result from vigorous rubbing and scratching. Disruption of the skin barrier puts the patient at risk for secondary bacterial invasion, primarily by Streptococcus pyogenes and Staphylococcus aureus. • Superinfection with S pyogenes can precipitate acute poststreptococcalglomerulonephritis and even rheumatic fever. • More common pyodermas include impetigo and cellulitis, which may rarely result in sepsis. Scabies infestations can exacerbate underlying eczema, psoriasis.
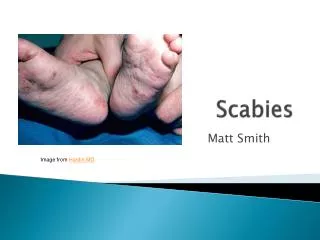
Manifestation • Lesion distribution differs in adults and children. • Adults manifest lesions primarily on the • flexor aspects of the wrists, • the interdigital web spaces of the hands, the dorsal feet, • axillae, • elbows, waist, buttocks, and • genitalia. • Pruritic papules and vesicles on the scrotum and penis in men and areolae in women are highly characteristic.
2.Infants and small children develop lesions predominantly on the • face, • scalp, • neck, • palms, and soles, • although any site may be involved. • All cutaneous sites are susceptible in immunocompromised and elderly patients, who often have a history of a widespread, pruritic eczematous eruption. • Consider the diagnosis of scabies in any patient presenting with a recent onset of intense itching that is accentuated at night.
Burrows are a pathognomonic sign and represent the intraepidermal tunnel created by the moving female mite. They appear as serpiginous, grayish, threadlike elevations ranging from 2-10 millimeters long. They are not readily apparent and must be actively sought. A black dot may be seen at one end of the burrow, indicating the presence of a mite. • Locations for burrows include the • webbed spaces of the fingers, • flexor surfaces of the wrists, elbows, axillae, • belt line, feet, • scrotum in men, and areolae in women. In infants, burrows are commonly located on the palms and soles.
Secondary lesions: • These are the result of scratching, secondary infection, and/or the host immune response against the mites and their products. • Characteristic findings include excoriations, widespread eczema, honey-colored crusting, postinflammatoryhyperpigmentation,postscabietic nodules.
Norwegian scabies. • Crusted scabies, previously referred to as Norwegian scabies, manifests with marked thickening and crusting of the skin. Lesions are often hyperkeratotic, crusted, and cover large areas. Marked scaling is common, and pruritus may be minimal or absent. Nail dystrophy and scalp lesions may be prominent. Predominantly affected are those with immunosuppression, neurological disorders, or institutionalization.
Investigation • Skin scraping: Place a drop of mineral oil on a glass slide, touch a No. 15 blade or a 7-mm curette to the oil, and scrape infested skin sites, preferably primary lesions such as vesicles, papules, and burrows .The skin scrapings are placed on a glass slide, covered with a coverslip, and examined under a light microscope • Add 10% potassium hydroxide (KOH) to the skin scraping. This dissolves excess keratin and permits adequate microscopic examination.
Treatment includes administration of a scabicidal agent, an antipruritic agent such as a sedating antihistamine, and an appropriate antimicrobial agent if secondarily infected. • All family members and close contacts must be evaluated and treated, even if they do not have symptoms • All carpets and furniture should be vacuumed and vacuum bags immediately discarded. • Patients with crusted scabies or their caregivers should be instructed to remove excess scale to allow penetration of the topical scabicidal agent and decrease the burden of infestation. This can be achieved with warm water soaks followed by application of a keratolytic agent such as 5% salicylic acid .
Scabicidal drugs • Gamma benzene hexachloride,1% -1 application • Benzyl benzoate25%-3 application for 12hrly interval • Lindane • Malathion • Permethrin,5%-1 application of 12hr Technique of application: • Apply the lotion or cream to the affected body surface from the neck down. • Leave the lotion for 12 hours . • And then wash off in shower. • If hands are washed out during this period then reapply the lotion or cream • A repeat of this after 1 week is someimes suggested . • Clothing and bedding is laundered.
Microscopic view of sarcoptes Burrows over the wrist
Burrow Norwegian scabies
Also known as lice infestation. • Lice are flat ,wingless blood sucking insects. • They lay eggs on hairs and clothings . • Two types of lice are responsible for the disease in human :pubic louse and body louse(scalp louse is the variant of body louse)
Infestation with head louse, Pediculushumanuscapitis, is common and highly contagious
Common among school childrens and more common in those who live in unhygenic and or poor social conditions. • Mode of transmission is by head to head contact .pubic louse are transmitted through sexual contact. Can be transmitted by infested clothings or beddings.
Clinical presentation • Itching :usually starts from the sides and back of scalp .scrating result in excoriation and secondary bacterial infection,cervical lymphadenopathy • If chronic infestation then lichenification and pigmentation can be seen .
The diagnosis is confirmed by identifying the living louse or nymph on the scalp or on a black sheet of paper after careful fine-toothed combing of wet hair that has had conditioner applied. • The empty egg cases ('nits') are easily seen along the hair shaft. These are characteristically difficult to dislodge.
Treatment • Malathion/permethrin • Carbaryl lotion applied to scalp/whole body for 12 hors and then wash the hair and repeated in 7 days . • Nits are removed with combs. • Clothing should be cleaned with hot water or even insecticides in some cases . • Sexual partners should also be treated.