Download
1 / 49
580 likes | 1.71k Views
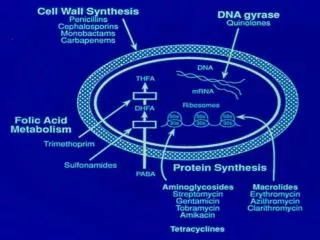
Beta lactam antibiotics. These are antibiotics having a Beta- lactam ring. The two major groups are penicillins and cephalosporins . Monobactams and carbapenems are relatively newer additions. BETA LACTAM CHARACTERISTICS. Same Mechanism of Action : Inhibit cell wall synthesis

E N D
These are antibiotics having a Beta-lactam ring. • The two major groups are penicillinsand cephalosporins. • Monobactams and carbapenems are relatively newer additions.
BETA LACTAM CHARACTERISTICS • Same Mechanism of Action : Inhibit cell wall synthesis • Bactericidal (except against Enterococcus sp.); time-dependent killers • Short elimination half-life • Primarily renally eliminated • Cross-allergenicity - exceptAZTREONAM
MECHANISM OF ACTION • Interfere with cell wall synthesis by binding to penicillin-binding proteins (PBPs) which are located in bacterial cell walls • Inhibition of PBPs leads to inhibition of peptidoglycan synthesis→ Cell death
PENICILLINS • Penicillin was the first antibiotic to be used clinically in 1941. It is a miracle that the least toxic drug of its kind was the first to be discovered. • It was originally obtained from the fungus Penicilliumnotattum, but the present source is a high yielding mutant of P. chrysogenum
Alexander Fleming discovered penicillin in 1928 • Alexander Fleming isolated the antibiotic substance penicillin from the fungus Penicilliumnotatum on September 15, for which he shared a Nobel Prize in 1945. • Penicillin is a antibiotic used in the treatment of bacterial infections caused by susceptible organisms
The structure of the penicillins consists of a thiazolidine ring connected to a beta-lactam ring, which is attached to a side chain. • All penicillins are derived from 6-Aminopenicillanic acid. • The various penicillinsdiffer in their side chain structure
Penicillins are divided into natural and semisynthetic one (antistaphylococcal, extendedspectrumpenicillins et .al) • Natural penicillins: extracted from the cultural solution of penicillia. • Prototype is penicillin G • Is pH sensitive. Therefore not given orally. • Effective against Gram-positive cells • Susceptible to penicillinase
CLASSIFICATION • Narrow spectrum penicillins • Beta lactamase sensitive(natural penicillins) • Acid stable penicillin-V/phenoxymethyl penicillin (oral) • Acid labile penicillin-G/benzyl penicillin (I.M, I.V), procaine penicillin –G (I.M, depot), benzathine penicillin-G (I.M, depot) 2. Beta lactamase resistant (antistaphylococcal) • Acid stable cloxacillin (oral, I.M), dicloxacillin (oral, I.M), flucloxacillin (oral, I.M) • Acid labile methicillin (I.M, I.V), nafcillin (I.M, I.V)
Extended spectrum Pns(all are sensitive to beta-lactamase degradation) • Acid stable (aminopenicillins) ampicillin (oral/parenteral), bacampicillin(oral/parental), talampicillin(oral/parenteral), amoxycillin(oral/parenteral) • Acid labile (antipseudomonalPns) carbenicillin, ticarcillin, piperacillin, mezlocillin, azlocillin(all parenteral)
ACID STABLE- PENICILLIN V • The oral form of penicillins • Indicated only in minor infections because of their relatively poor B/A, weaker antimicrobial activity, the need for dosing many times • NARROW ANTIMICROBIAL SPECTRUM.
ACID LABILE-PENICILLIN G • It is relatively unstable in acid, thus the B/A is low. • Suitable for I/M or I/V admn. • A single 6Lac unit I/M dose of procaine Pn yields clinically effective concentrations for 12-24hrs DOC- syphilis,neurosyphilis
Single I/M dose of 1.2million units of benzathinePn-G can provide plasma levels which are sufficient to protect against beta-haemolytic streptococcal infection for 3weeks( longest acting)
There is poorpenetration into the cerebrospinal (CSF), unless inflammation (meningitis) is present. • Pn-G is excreted by the kidneys, its elimination occurs via tubular secretion while only 10% is excreted by glomerular filtration • Probenicidblocks tubular secretion of Pn
SPECTRUM OF ACTIVITY & USES • Gm +vecocci: strep pyogenes (pharyngitis, otitis media), strep pneumoniae, strep viridanss & strep faecalis i.e., enterococcus (SABE) • Simultaneous administration withgentamicinto treat enterococcalendocarditis • Single injection of benzathinePn-G is satisfactory for treating rheumatic fever as it prevents colonisation of beta haemolytic streptococci
Gm +ve bacilli: • DOC for tetanus (C tetani), gas gangrene (C perfringes), diphtheria (C diphtheriae), anthrax (Bacillus anthraecis), meningitis (l monocytogenes) • Spirochetes like T Pallidum (syphilis) are highly sensitive. BenzathinePn-G (2.4MU I.M once a wk for 2-3weeks)
Pn-G is moderately active against gm –vecoccisuch as N meningitidis (menigitis) & N gonorrhoeae (gonorrhoea) • also active against Actinomyceteslike actinomycesisraelii(cranio-facial/thoracic/abdominal abscess)
ANTISTAPHYLOCCAL PENICILLINS • Narrow spectrum, beta lactamase resistant (cloxacillin, dicloxacillin, methicillin, nafcillin) • Methicillin is no longer used because of nephrotoxicity. Nafcillin is preferred for parenteral use while cloxacillin & dicloxacillin can be given orally
Osteomyelitis, septicaemia, endocarditis & cellulitis c/b susceptible strains of staphylococci • Cloxacillin in addition can also be used to treat mild staphylococcal skin infection such as impetigo
BROAD SPECTRUM PENICILLINS Ampicillin and amoxycillin(aminopenicillins) • Both have adequate oral B/A, ingestion of food decreases the B/A of ampicillin so must be administered 1hr before or after meals Bacampicillin & talampicillin are prodrugs of ampicillin, disturb intestinal flora to much lesser extent
They are similar to penicillin G in the activity against gram-positive organisms but are weaker than the latter. • They are more satisfactory for the treatment of enterococciand streptococcus viridians
They are similar to chloramphenicol in the activity against gram-negative organisms (B pertusis, H Inflenza, E coli, S typhi, P mirabilis & Shigella) • Amoxycillin is also used in multidrug regimens for eradication of H pylori in duodenal & gastric ulcers
Ampi & amox are also very effective against strep viridans & enterococci(SABE) & pneumococci • For SABE, ampicillin 2g I.V every 6hrs may be used in place of Pn-G • Ampicillin is also effective in meningitis c/b L monocytogenes
They are acid-resistant but are not penicillase-resistant. • P. aeruginosa are fail to respond to these drugs.
ANTIPSEUDOMONAL PENICILLINS • Carboxypenicillins(carbenicillin & ticarcillin) • ureidopenicillins (piperacillin, mezlocillin, azlocillin) are acid labile
Piperacillin have comparable spectra of activity against many gm +ve & gm –veorganisms, special feature is their activity against P aeruginose & indole +ve Proteus which are not inhibited by Pn-G or aminopenicillins
Used for serious infections due to pseudomonas, proteus, klebsiella as in burns, septicaemia, UTI & in immunocompromised patients. • Generally used in combination with an aminoglycoside(gentamicin) for pseudomonal infections.
BETA LACTAMASE INHIBITORS • Resemble b-lactam antibiotics only structurally but do not possess any significant antimicrobial action • They bind irreversibly to the catalytic site of susceptible b-lactamases (produced by bacteria) to prevent hydrolysis of Pns(SUICIDE INHIBITORS) • They can inhibit plasmid mediated b-lactamaseswhich are responsible for transferred drug resistance
CLAVULANIC ACID (derived from streptomycesclavligerus), SULBACTAM (semisynthetic) & TAZOBACTAM (structural analogue of sulbactam)
Only clavulanic acid is orally absorbed, others are used parenterally • They are available in FDC • clavulanic acid is combined with amoxycillin • sulbactam with ampicillin • tazobactam with piperacillin
Addition of clavulanic acid with amoxycillinextends the antimicrobial spectrum of amoxycillin against b-lactamase producing bacteria like strep pneumoniae, H influenzae& moraxella(otitis media, sinusitis, RTIs), methicillin sensitive staph aureus, K pneumoniae(nosocomialPneumoniae), penicillinase producing N gonorrhoae, b-lactamase producing anaerobes, E coli, Proteus
Amoxycillin 250/500mg + clavulanic acid 125mg tablets/capsules
Ampicillin 1g + sulbactam 0.5g; I.V/I.M • Piperacillin 2g + tazobactam 0.25g; I.V/I.M • Adverse effects are rare except GI intolerance, stomatitis & rashes
RESISTANCE TO PENICILLINS 1. production of β-lactamase enzymes • most important and most common • hydrolyzes beta-lactam ring causing inactivation 2. Trapping mechanism. • Some b -lactams tightly bind with b -lactamase and stay outside the bacterial cell. Thus, these beta-lactams can’t enter the bacterial cell wall to combine with the PBPs.
3. Modification of target PBPs. • responsible for methicillin resistance in staphylococci and penicillin resistance in pneumococci. 4. Impaired penetration of drug to target PBPs. • which occurs only in Gm -ve species, is due to impermeability of the outer membrane that is present in Gm -ve but not in Gm +ve bacteria.
5. The shortage of autolytic enzyme. • Under this circumstance, the beta-lactams have normal inhibiting action, but their kill effects are very poor. 6. The presence of an efflux pump. • Some organisms also may transport betalactam antibiotics from the periplasm back across the cell wall via an efflux pump
ADVERSE EFFECTS • Hypersensitivity reactions – 5 to 20 % • Immediate HS reactions – m/c & occur within 20min of parenteral administration • Urticaria, pruritis, wheezing, sneezing, rhinitis – may pass over toanaphylaxis c/b diffused pruritis, hypotensive shock, angioneuroticedema, choking, l/o of consciousness & death • Adrenaline (s/c or i/m), corticosteroids (i/v or i/m), antihistamines (i/m), O2 inhalation, i/v fluids or plasma expanders
Accelerated HS reactions usually occur within 72hrs • Rash, fever, urticaria but rarely angioneuroticedema, fatality is extremely rare • Late HS reactions occur after 72hrs • Morbiliform, urticarial or erythematous eruptions, local inflammatory reactions, lymphadenopathy, splenomegaly, serum sickness
2. GASTROINTESTINAL diarrhoea is more common with ampicillin, • glossitis, • stomatitis, • abnormal • taste • sensation
3. NEPHROTOXICITY, is very rare. 4. SUPERINFECTIONS, results from alterations in intestinal flora. A higher incidence occurs with broad-spectrum penicillins. 5. Pn injected in a syphilitic patient may produce Jarisch-Herxheier reaction c/b fever, myalgia & even collapse d/t sudden release of spirochaetal breakdown products which may last upto 72hrs
DRUG INTERACTIONS • ANTAGONISTIC COMBINATIONS • Oral Pns may be antagonised by bacteriostatic antibiotics (tetra, chloram, erythro) as they will diminish bactericidal effect of Pns by inhibiting the bacterial growth • Pns & AG’s should not be mixed in same syringe as they inactivate each other • Ampicillin with allopurinol may cause non-urticarialmaculopapular rash • Hydrocortisone inactivates ampicillin if mixed in the I/V fluid
SYNERGISTIC COMBINATIONS • Probenecid prolongs the action of Pn by decreasing its tubular secretion • Procaine Pn-G with gentamicin against strep viridans, strep faecalis in SABE • Piperacillin & gentamicin against Pseudomonas & proteus • FDC of ampicillin/amoxycillin with cloxacillin in postoperative & respiratory infections.