Download
1 / 84
1.23k likes | 1.84k Views
CBRN Disaster Management. Dr. Rakesh Kumar Sharma Additional Director, Institute of Nuclear Medicine and Allied Sciences, Delhi. @Training Programme on Chemical (Industrial) Disaster Risk Management, 27-28 August 2010. All-Hazards. Natural Earthquake Landslides Floods Fires etc….

E N D
CBRN Disaster Management Dr. Rakesh Kumar Sharma Additional Director, Institute of Nuclear Medicine and Allied Sciences, Delhi @Training Programme on Chemical (Industrial) Disaster Risk Management, 27-28 August 2010
All-Hazards • Natural • Earthquake • Landslides • Floods • Fires etc… • Human-made • Fires • Explosive devices • Firearms • Structural collapse • Transportation event • Air, Rail, Roadway, Water • HAZCHEM / HAZMAT • WMD • CBRN events • etc…
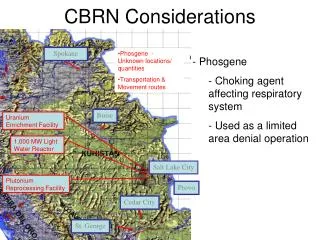
CBRN Terrorism Threat: Fact or Fiction? Radiological: trafficking in radio-isotopes but no incidents Nuclear: trafficking in plutonium and highly enriched uranium – but no incidents with improvised, stolen or sold nuclear device Chemical: Sarin attack in Tokyo’s subway system in April 1005: 12 killed, dozens wounded Biological: Anthrax attack in USA 2001: 5 killed, 22 infected
The Fukushima Daiichi nuclear was an at the Fukushima Nuclear Power Plant in Fukushima. Following earthquake on 11 March 2011. Active reactors automatically shut down their sustained fission reactions. However, the tsunami disabled the emergency generators that would have provided power to control and operate the pumps necessary to cool the reactors..
The insufficient cooling led to three nuclear meltdowns, hydrogen-air explosions, and the release of radioactive material in Units 1, 2, and 3 from 12 March to 15 March. Loss of cooling also caused the pool for storing spent fuel from Reactor 4 to overheat on 15 March due to the decay heat from the fuel rods
The Fukushima disaster was the most significant nuclear incident since April 26, 1986 the Chernobyl disaster and the second disaster to be given the Level 7 event classification of the International Nuclear Event Scale.[ According to the linear no-threshold theory of radiation safety, that will be caused by the accident is expected to be around 130–640 people in the years and decades ahead.[ However, an estimated 1,600 deaths are believed to have occurred due to the resultant evacuation conditions
The Matsumoto sarin attack was an attempted assassination perpetrated by members of the Aum Shinrikyo doomsday cult in Matsumoto, on the night of June 27, 1994. Eight people were killed[1][2] and over 200 were harmed by sarin gas that was released from a converted refrigeration truck in the Kaichi Heights area. The attack was perpetrated nine months before the better known Tokyo subway sarin attack. The gas attack occurred in a quiet residential area in the city of Matsumoto in Nagano Prefecture. Aum Shinrikyo had two goals; to attack three judges who were overseeing a lawsuit concerning a real-estate dispute which was predicted to go against the cult, and to test the efficiency of its sarin — which the cult was manufacturing at one of its facilities — as a weapon of mass-murder.[3] The citizens of Matsumoto had angered Aum Shinrikyo founder Shoko Asahara by vigorously opposing his plan to set up an office and factory on land in southern Matsumoto. Opponents of the plan gathered 140,000 signatures on an anti-Aum Shinrikyo petition, equivalent to 70 percent of the city’s population at the time.[4]
‘New’ Elements in ‘ New Terrorism’ • Attempts to acquire Weapons of Mass Destruction • Religious Fanaticism • Catastrophic Terrorism • Border Porosity • Global Communication • Expansion of Range of Targets (Tourists, ICRC, UN) • Links with Organized Crime • New Sources of Financing • Failed and weak states as de facto safe havens
EmergencyVs.Disaster A SUDDEN HAPPENING WHICH REQUIRES PROMPT ACTIONS A SUDDEN& MASSIVEHAPPENING WHICH REQUIRES PROMPTAND HUGEACTIONS
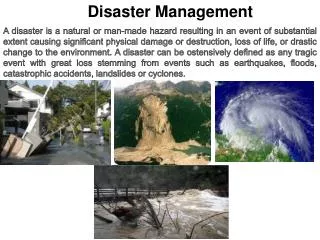
Disaster- dis·as·tern. • An occurrence causing widespread destruction and distress; a catastrophe. • A grave misfortune. • Informal- A total failure
‘Disaster’ Definition • A disaster is present when need exceeds resources! • ‘Response need’ > ‘Response available’!
The DISASTER Paradigm D: Detection I: Incident Command S: Safety & Security A: Assess Hazards S: Support T: Triage & Treatment E: Evacuation R: Recovery
What is CBRN? • CBRN is an acronym referring to • Chemical, • Biological, • Radiological, and • Nuclear threats • It is in common use worldwide, generally to refer to PROTECTIVE MEASURES taken against CBRN weapons or hazards.
….. Twenty years ago CBRN Technologies …..Today Access to Technology in hands of terrorists Force Multipliers : Connections (good networking amongst themselves as well as with rogue nations) Terrorist organizations are Faster and Flexible Requires Force Multiplication for Antiterrorism, Reaction and Response Technologies Requires New Ways/Paradigms of Thinking Technologies Approach Great Technology in the hands of NATIONS Conventions in place Mainly in Military domain Military Intelligence input and War Gaming Defence Preparedness Prediction technologies
Terrorist Tactics, based on 25,303 terrorist events, 1968-2004 % of all events % of all casualties Bombs 53.4 70.1 Guns 19.9 23.0 Arson 9.8 2.7 Remote control bombs 1.9 4.7 Knives & other blades 1.3 2.1 Chemical 0.2 0.59 Biological 0.08 0.02 Other 13.3 8.1 Total 100.0 100.0 Source: p.49.Kenneth T. Bogen and Edwin D. Jones. Risks of Mortality and Morbidity from Worldwide Terrorism: 1968-2004. Risk Analysis Vol. 26, No.1, 2006. – Data utilized are from RAND-MIPT. Incidents until 1997 include only international terrorism.
List of probable agents for terrorist Attack(in descending order of likelihood) Use of a conventional explosive Release of an industrial chemical Release of a military chemical agent Use of a ‘dirty’ bomb Release of a biological agent Detonation of a nuclear device Sharp et al. Ann Em Med;32(2):214 (1998) CDC Science & Technology Center
CBRN Emergencies are Happening We are as much a target as any other ………… …. don’t happen to places ….. happen to people ……can happen to us! Disruption
Terrorist Groups and Unconventional Weapons High C CR CRB CRBN Al Qaeda LTTE Danger AUM Hizbollah FARC (?) HAMAS (?) DHKP/C (?) PKK (?) BKI RIRA ETA MILF AUC IMU N17RO SL ASG Kach Chechen Rebels PIJ GSPC GIA Low High Sophistication of Unconventional Weapons
Table 29 : Homeland Security Planning Scenarios 2004 1. Nuclear Detonation Can vary widely 2. Biological Attack 13,000 fatalities & injuries 3. Biological Disease Outbreak (Pandemic Flu) 87,0000 fatalities, 300,000 hospitalized 4. Biological Attack – Plague 2,500 fatalities;7,000 injuries 5. Chemical Attack – Blister Agent 150 fatalities; 70,000 hospitalized 6. Chemical Attack –Toxic Indust. Chemicals 350 fatalities;1,000 hospitalizations 7. Chemical Attack – Nerve Agent 6,000 fatalities; 350 injuries 8. Chem. Attack –Chlorine Tank Explosion 17,500 fatalities; 10,000 injuries 9. Radiological Attach – RDD 180 fatalities;20,000 contaminations 10. Explosive Attack IED Bombing 100 fatalities; 450 hospitalizations 11. Biological attack – Food Contamination 300 fatalities; 400 hospitalizations
The Impact Leaves a long trail of sufferings Profound sufferings – beyond the range of normal human experience Impact is multi pronged Physical, Psychological, Economical, and Social
The Resultant Worst case scenario is much more threatening • Psychological vulnerability and Neuropsychological Sequelae • Fear of unknown • Fleeing of affected community • Exponential spread of disaster victims • Overwhelming of hospitals by people believing themselves to be affected • Hoardings • Decreased efficiency of system • Collapse of civil disorder and essential services • …feeling of Powerlessness, …., ….., …..
CHAOS at the Incident Site • are inevitable • can not be PREVENTED • TRY to Reduce chaos ASAP • Organise the CHAOS
The Expectations • …………….knee jerk reactions
The Expectations • …………….knee jerk reactions • Overall Preparedness and Risk Reduction at all levels • Contingency Planning Abilities • Capacity development • Infrastructure • Trained Human Resources • Attitudinal Changes
The Expectations • …………….knee jerk reactions • Overall Preparedness and Risk Reduction at all levels • Contingency Planning Abilities • Capacity development • Infrastructure • Trained Human Resources • Attitudinal Changes • Coordination Issues
‘When a disaster strikes, the Community (general population) expects branches of local, state, and Central government and NGOs to rapidly mobilize to help the impacted community.’
Disturbing Trends of Disaster The Sarin gas attack on the Tokyo subway, usually referred to in the Japanese media as the subway sarin incidentwas an act of domestic terrorism perpetrated by members of Aum Shinrikyo on March 20, 1995.
Genie out of the bottle VERTEX OF EVIL 30 120 Disturbing Trends of Disasters Chemicals are toxic manmade compounds including those designed for warfare use or industrial use TOI dated 21st February 2007
Disturbing Trends of Disasters • Chlorine bombings in Iraq began in January 2007, when insurgents in Al Anbar province started using chlorine gas in conjunction with conventional vehicle-borne explosive devices. • Low level exposure results in burning sensations to the eyes, nose & throat, usually accompanied by dizziness, nausea and vomiting. Higher levels of exposure can cause fatal lung damage; and so it is generally considered ineffective as an improvised chemical weapon.
When evil minds combine,Good minds have to work together and combat. NDMG CD CHEMICAL TERRORISM
We have to be lucky all the time. They have to be lucky only once!!! When planning, think more than a terrorist! When implementing, think as a ‘poor’ victim!
Chemical Use by a Non-State Group or Individual • A non-state group or individual pursuing a chemical weapons capability is more likely to choose Industrial Chemicals; such agents are generally easier to handle and produce and require less specialized production equipment than do Chemical warfare agents.
What is the goal of the Terrorist? • If the goal is to kill a single person or small group, there are chemical agents that can accomplish a murder on a small scale. • For example, Ricin, produced from castor beans kills by epidermal contact.
A Terrorist’s Goal may be Mass Murder • This objective is the most suitable for dissemination of a Toxic Industrial Chemical or a Chemical Weapon • Chlorine is readily available. Disseminated in a closed, positive air pressure environment, it could get into the lungs of most people in the environment. In other settings, however, the difficulties of spreading chlorine outdoors and the unlikelihood of it spreading from one victim to another render it a poor open-air, urban-devastating weapon. • CW agents carry the most potential to spread quickly and cause more casualties and panic
Scale for Grading of Chemical Disasters Grades Qualitative Severity/ Consequence Criteria 1 • Injuries requiring first-aid only • Contained release with local environmental effect and pollution problem 2 • Injuries requiring a physician’s care • Uncontained release with potential for minor environment effects • Chances of fire and explosion 3 • Severe injuries or potential for a fatality • Uncontained release with potential for moderate environment effects 4 • Multiple life threatening injuries and / or fatality • Uncontained release with potential for major environment effects
Gaps ……Recognition While considerable progress has been made in the last two decades in the development and implementation of regulations and programmes for the management of chemical disasters, salient gaps still exists in certain areas ……. BETWEEN THE CAPACITIES OF THE VARIOUS AUTHORITIES, LEGISLATION AND ACTUAL REQUIREMENT DURING A DISASTER
NDMA • Mandated to laying down policies, plans and guidelines for the Nation, State, Ministries and departments (Under Section 6 of the Disaster Management (DM) Act, 2005 • State, Ministries and departments shall prepare plan for preparedness and response • The National and State Disaster Management Plans will finally be approved by NDMA and respective SDMA as specified in Section 11 and Section 23- subsection 3 of DM Act, 2005 respectively • NDMA to coordinate and ensure implementation of the guidelines and plans (Section 35 seeks to enjoin upon the Central Government, as it deems necessary or expedient, for the purpose of disaster management)
The role of NDMA and Govt. The main goal of NDMA and ministries in the Central Government will be to promote the cooperation between the different sections of the government, stakeholders and the society for the promotion of Chemical Disaster-Resilient Society and the implementation of CDM action plan
National Disaster Management Guidelines- Management of Chemical (Terrorism) Disasters
Modes of Chemical Injury • Chemical Burns (strong acids, strong bases) • Heat Burns (flammable materials) • Poisoning (many chemicals are damaging or fatal if taken internally, whether by swallowing, injection, or leaching through skin) • Chronic illness (long-term exposure to even low doses of certain chemical agents can lead to chronic health conditions) • Etc.
General Signs and Symptoms • Cough • Chest pain • Lacrimation • Eyelid oedema and • Unconsciousness Acute lung injury Leads to Cardiac arrest DEATH
TARGET ORGANS AND EFFECTS INDUCED BY CHEMICALS Corneal Opacity Retinal Damage Behavior Changes Peripheral neuro degeneration Locomotion rigidity Narcosis or Depression Respiratory Paralysis Osteoporosis Arthritis Immuno Suppression Corrosiveness Erythemas Irritations Sensitization Pneumoconiosis Fibrosis Adenomas Asphyxiation MFO induction Choleostasis Carcinogenesis Necrotic/Cirrhotic liver Defense system loss Aminoacid urea Uremia Renal failure Bone marrow depression Anaemia Cancer Met hemoglobinemia Miscarriage Neonatal death Fetal abnormalities
Chemical Disaster Action Plan Gather information regarding: place, time and type of emergency also type of chemical, chemical toxicity, route of exposure OT Treatment to the patient (Emergency Dept.) Decontamination done at decontamination area in the hospital Triage IPD / ICU Documentation done at reception OPD • Mobilization of Resources • Manpower: Disaster Management Team medical , nursing and other Personnel • Material and supply eg: antidotes • Transportation means Transport to the critical patients for medical care / hospitals Discharge Getting initial alert from: Police, casualty and telephone • Initiate preparation • All the dept & designated staff get into readiness to attend casualties • Crisis expansion of hospital beds. • Preparation for decontamination area Notify to Key Personnel • Diagnostic Services • Other support services • On site treatment / operations • Mass decontamination • Transported in a safe place • Provide necessary treatment , first aid and antidote administration to chemical contaminated patients
Management of Chemical accident • Pre-hospital • Hospital • Post-hospital • Preventive