Download
1 / 21
230 likes | 535 Views
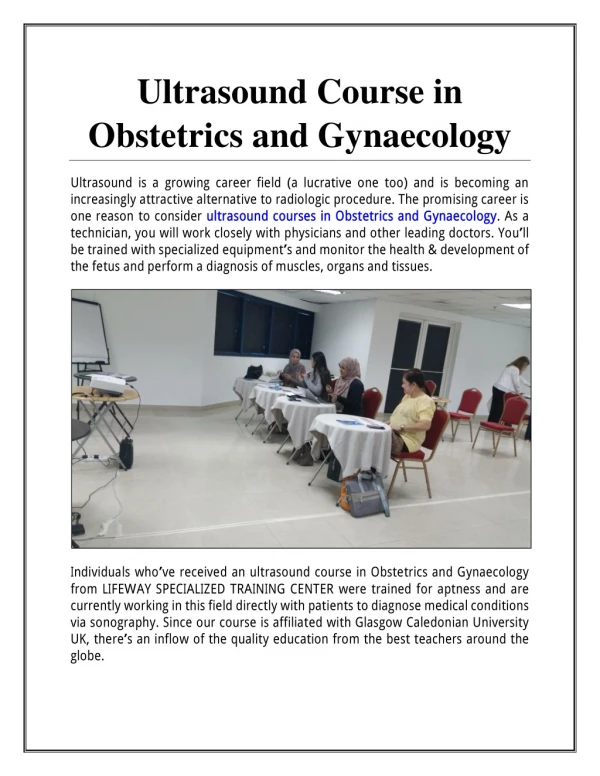
Ultrasound in gynaecology. By Dr. Khattab KAEO Assis. Prof. of Obstetrics and Gynaecology Faculty of Medicine, Al-Azhar University, Damietta. Introduction. Ultrasound has a frequency >20 000 Hz (20kHz). However, ultrasound machines have frequencies of 2-10 mega Hz (MHz).

E N D
Ultrasound in gynaecology By Dr. Khattab KAEO Assis. Prof. of Obstetrics and Gynaecology Faculty of Medicine, Al-Azhar University, Damietta
Ultrasound has a frequency >20 000 Hz (20kHz). However, ultrasound machines have frequencies of 2-10 mega Hz (MHz). • Higher frequencies give better resolution, but decreased tissue penetration; thus, used to examine near structures. Conversely, lower frequency probes are used to examine deep structures. For instance, abdominal probes give 3-5 MHz, while vaginal probes give 5-7.5 MHz. • It is best to reduce 'depth' as much as possible. • Increasing the 'gain' increases the echoes, and thus, may improve the image where obesity is causing attenuation.
TRANSABDOMINAL ADVANTAGES • View of entire pelvis. • Evaluate large masses. • Evaluate masses out of range of trans-vaginal probe. • Can be used in patients with intact hymen.
TRANSABDOMINAL DISADVANTAGES • Full bladder requires time for patient to fill and may cause pain during examination. • Some patients cannot adequately fill bladder. • Difficult to evaluate retroverted uterus.
TRANSVAGINAL ADVANTAGES • Proximity to pelvic organs with higher frequency transducer allows for better tissue characterization. • Empty bladder scanning typically is less painful than with a distended bladder. • Good for obese patients and patients with abdominal wall scars, which limit ability to scan transabdominally.
TRANSVAGINAL DISADVANTAGES • Limited field of view; masses out of the range of the transducer are missed. • Cannot be used in patients with intact hymen. • Some patients will not be comfortable with examination.
Abnormal uterine bleeding: An ill-defined echogenic region adjacent to the endometrium could be a fibroid, adenomyoma or a tumour.
Infertility • Ultrasound is the technique of choice for imaging the endometrial cavity & the ovaries • In the premenopausal women the ovaries are usually located overlying the internal iliac vessels, lateral to the uterine fundus, easily recognizable dueto the presence of numerous echoluscent follicles of varying diameters. When the ovaries are not immediately visualized, the operator can use his other hand to press on the anterior abdominal, as if performing a bimanual examination. Alternatively, shifting the patient to a different position may help. • When menopausal changes affect the ovaries they become smaller and the previously-mentioned sonographic markers become no more seen. Inability to visualize one or both ovaries is not unusual.
- With large uterine leiomyomas the ovaries usually become abdominal structures. Also, after hysterectomy the adnexal structures may be retracted out of the pelvic view. • - Ovarian dimensions predicted by TVS closely correlate with surgical findings. Ovarian volume is calculated by multiplying 0.5 x length x width x breadth. The volume is fairly constant at 6.6-6.7 cc until the age of 40. - Ovarian volumes persistently >20 cc premenopausal & 10 cc post-menopausal should be a cause of concern & prompt further investigation. • - During the normal menstrual cycle, ovarian morphology changes on a daily basis. It is important to recognise the synchrony that occurs between the ovary and endometrium.
- Initial follicular growth is hormone-independent & therefore, <5 mm follicles will be visible even in those women taking COCs. - Ultrasound is very valuable in monitoring ovulation induction & directing egg collection. - The follicular wall is initially well-defined with a clear sharp defining edge, becoming thicker and blurred as ovulation approaches. The cumulus oophorus may be visualized projecting into the follicle 2-3 days prior to ovulation. - Ovulation results in disappearance of the dominant follicle, along with some free fluid in the pouch of Douglas. - The corpus luteum morphology could be cystic or solid. Its internal walls may be irregular. - Haemorrhgic corpora lutea often demonstrate fine synechiae forming a network within a cyst.
Classic appearance of haemorrhagic ovarian cyst. Differential diagnosis: Corpus luteum cyst (occupies the mid-portion of the ovary).
# Empty gestational sac: Some are viable, while others represent blighted ovum. The mean sac diameter (MSD = the mean of 3 perpendicular measurements), rather than volume, is the key for management. MSD 20mm = home & re-scan in 7-10 d. MSD >20 mm = termination of pregnancy. You should look for a second opinion.
Empty gestational sacs (absent embryo, even if amniotic sac is seen [arrow]). Arrow heads point to thin decidual reaction. The lowermost sonogram shows an abnormally large yolk sac, presented for comparison with the first one sonogram.
# Retained products of conception: Mixed echogenicity with irregular echo-bright areas (it is difficult to differentiate blood clots from retained tissues). Mostly the tissue is of <30 mm maximum diameter with light blood loss and no signs of infection, and so, management is conservative. Large volume of tissue or heavy blood loss = evacuation.
# Empty uterus: Differential diagnosis: 1- very early pregnancy; 2- complete miscarriage; or 3- ectopic pre gnancy. Consider: 1- history for risk factors for ectopic pregnancy, 2- examination findings and 3- -hCG level as well as its rate of disappearance. If tissues have been passed, this should be examined microscopically for chorionic villi. When -hCG level exceeds 1000 iu/l, intrauterine pregnancy would be visible by TVS (5000 iu/l for TAS). -hCG level is the key for management. A- -hCG <1000 iu/l: All the 3 possibilities are probable. If there are no risk factors for ectopic pregnancy and no peritonism, review after 48 hours by TVS and -hCG. The absolute level of -hCG (1000IU/L) should be relied upon rather than the rate of rise in -hCG level. Some ectopic pregnancies (13%) show normal rate of -hCG rise. Some normal pregnancies (15%) show slow rate of -hCG rise. (Between the 2nd & 4th post-ovulation weeks the level of -hCG doubles every 48 hours; ectopic pregnancy and abortion shows <66% rise). B- -hCG 1000 IU/L, only ectopic pregnancy or complete abortion are possible. Laparoscopy can be considered or selectively with review in 48 hours. Complete abortion can be confirmed by a -hCG fall to 20% by 48 hours. History may assist decision-making. Regarding the disappearance rate of hCG: if it is less than 1.4 days, the most likely diagnosis is miscarriage. If it is greater than 7 days, the case is almost always ectopic pregnancy.