Download
1 / 22
240 likes | 482 Views
I’ve got a bit of a headache. GWR Presentation. James ng. history 1. 31 Indian. Male. IT manager for SPF. Slightly overweight 2/52 Headache Constant R + posterior pain. Radiates forward Worse with changes in posture Present on waking but does not actually wake him

E N D
I’ve got a bit of a headache... GWR Presentation James ng
history 1 • 31 Indian. Male. IT manager for SPF. Slightly overweight • 2/52 Headache • Constant R + posterior pain. Radiates forward • Worse with changes in posture • Present on waking but does not actually wake him • 1/7 Came to ED. Discharged. CT not done • This AM: • Re-attendance for headache. Headache more painful • Also, woke up with a black line in R vision • Horizontal, mobile, across central vision • ? R vision more blurred- not sure • L eye OK • No head injury/ foreign travel/ infection/ FH etc
history 2 • ROS • 2/12 lumps on L side of neck, disappeared after 1/12 • 3/52 lump under L armpit, disappeared after 3-4/7 • 3/7 lump under R armpit- started on antibiotics by polyC • Recently, had a few small bruises on R shoulder from carrying shoulder bag • No fevers/ night sweats • Blood donor, last donation Dec 2007 • Social • Married for 7 yrs, 1 partner • Some SOB recently, so tried to take up running again. ET: 300m. Used to go on runs 6/12 ago
examination- eye • Vision with glasses: R 6/5 L 6/4 • IOP: 18 18 • Normal anterior segments • No RAPD • Minimal cataract • .. DBE
Roth’s spots- a misnomer • 1872, Moritz Roth described small white spots on the retina associated with separate areas of ret h’ge in septic patients • 1878, Moritz Litten reported that white centred h’ges were associated with endocarditis • ‘Roth’s Spots ‘ (now classically seen in endocarditis). • Strictly these h’ges should be called Litten’s sign • rupture of retinal capillaries with exudation of whole blood, followed by platelet fibrin thrombus formation (the pale white centre). • History did not look kindly upon Litten: • Litten was also the 1st physician to describe vitreous bleeding assoc. with subarachnoid h’ge (not Albert Terson!)
differential diagnosis Blood disorders Anaemia/ thrombocytopenia/ MM Leukaemia Scurvy Infective Endocarditis: bacterial/ fungal Sepsis AIDS retinopathy Candida retinopathy Vasculitis DM Systemic Vasculitis (SLE, etc) Other Hypertension Carbon monoxide poisoning OCP Birth trauma Prolonged intubation
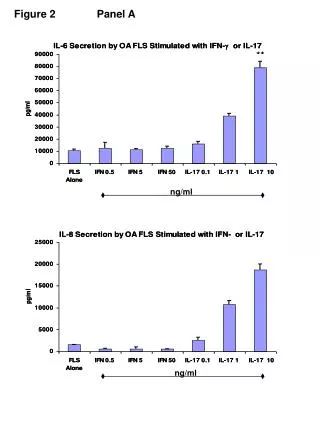
Figure 1. Behcet's disease with multiple systemic thrombotic manifestations (notice disk involvement) Figure 2. Idiopathic aplastic anemia (WBC 200; Hb 5.9; Plt 6000)
Figure 3. Acute myeloblastic leukaemia Figure 4. A 40-year-old woman with rheumatic heart disease and Streptococcus viridans endocarditis Three lesions demonstrate, from left to right, evolution of a Roth spot
.. the rest of the examination • Pale tarsal conjunctiva • Petechial bruising on: • R shoulder and back • Around L arm just above the elbow • Rubber nodules: • 3x 6 cm in R axilla • Trace nodule in R groin • NAD • Hands, CVS, Resp, Abdo, Neuro
working diagnosis • Infective Endocarditis • Autoimmune/ embolic phenomenon • Haematological malignancy • HIV/ Disseminated infection
management • Observe eye condition • Patient already referred to Neurology (from ED) • FBC, U+E, Clotting, ESR, CRP • if total white high, admit. • Blood cultures
blood results • Hb: 4.7 • WBC: 39.6 • PLT: 11 • Blasts: 75% • MCV: • ESR: 105 • CRP: 16.8 • Clotting: normal
what happened next? • Blood crossmatched • CT Brain normal, cleared by Neurology • 2 units transfused • Patient sent to NUH Haematology: • Acute Lymphoblastic Leukaemia
ALL Malignant disorder of lymphoid progenitor cells Most common leukaemia in children (2-5yrs) Adult ALL 15-25 yrs old and over 75 yrs Immunological classification: B or T cell type, influences Mx 75% are early (precursor) B-cell 20% of adult cases of ALL are T-cell in origin 5% more mature B-cells/ Burkitt-type ALL Cause: unknown, incr common in Hiroshima (post bomb) Rapidly fatal without treatment
diagnosis triad and investigations ‘Classic Triad’: anaemia, low platelets, ↑abN WBCs Diagnostic criteria: Blood count/film suggestive of leukaemia Lymphadenopathy persisting for > 6 wks Hepatosplenomegaly 3 or more: Fatigue, night sweats, weight loss, itching, breathlessness, bruising, recurrent infections, bone pain Other investigations: BM Biopsy for chromosome analysis (Ph, etc) Staging X rays and scans LP if CNS based Clotting (1/20 abN), and gen workup.
treatment To kill all the abnormal cells Main treatment is chemotherapy +/- combined with radioRx +/- stem cell transplants 3 phases: Induction remission phase- an initial intensive Rx to achieve being ‘in remission' Consolidation (Intensification) phase- kill undetectable cells Maintenance phase- less intensive, oral chemoRx + wkly injection
what happened after? • Just recently admitted to NUH • Now having 4th cycle of cytotoxics, awaiting BM donor • Can have a maximum of 8 cycles whilst a BM donor is sought
References PPomeranz. Roth Spots. Arch Ophthalmol.2002; 120: 1596 J S Pepose, G N Holland, M S Nestor, A J Cochran, R Y Foos Acquired immune deficiency syndrome. Pathogenic mechanisms of ocular disease. Ophthalmology. 1985 Apr ;92 (4):472-84 2987769 Ndoye NB, Sow PS, Ba EA, Ndiaye MR, Wade A, Coll-Seck AM. [Ocular manifestations of AIDS in Dakar][Article in French]Dakar Med. 1993;38(1):97-100 Turu AC, Civera AA, Latorre X. Ophthalmic manifestations of acquired immunodeficiency syndrome. A study of thirty-four patients. Ophthalmologica. 1988;197(3):113-9 Pui CH, Robison L, Look AT. Acute Lymphoblastic Leukemia.The Lancet, Volume 371, Issue 9617, 22 March 2008-28 March 2008, P 1030-1043