Download
1 / 25
260 likes | 557 Views
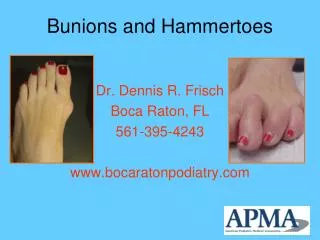
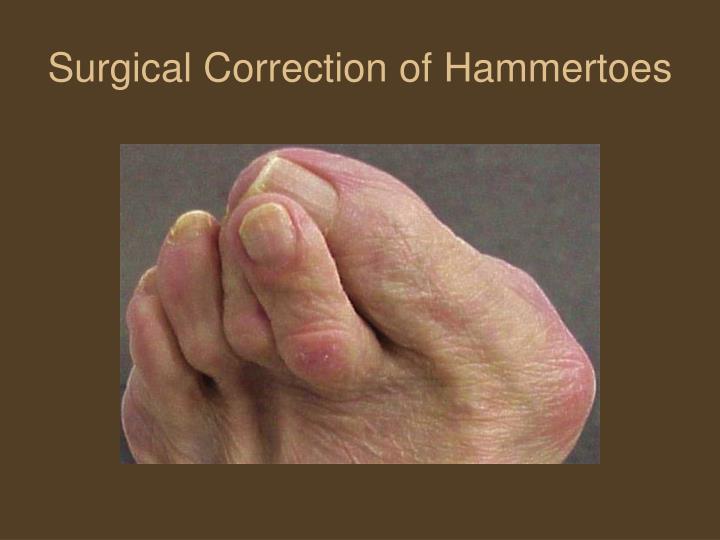
Surgical Correction of Hammertoes. What are Hammertoes?. Classic Hammertoe MPJ is cocked upward and PIPJ is downward Claw Toe MPJ is upward, PIPJ and DIPJ are downward Mallet Toe DIPJ is downward. What Causes Hammertoes?. Hammertoes are primarily caused by a muscle imbalance during gait

E N D
What are Hammertoes? • Classic Hammertoe • MPJ is cocked upward and PIPJ is downward • Claw Toe • MPJ is upward, PIPJ and DIPJ are downward • Mallet Toe • DIPJ is downward
What Causes Hammertoes? • Hammertoes are primarily caused by a muscle imbalance during gait • There is also evidence that poor fitting shoes can contribute
Extrinsic Muscles: Flexor Digitorum Longus Extensor Digitorum Longus Flexor Hallucis Longus Extensor Hallucis Longus Tibialis Anterior Tibialis Posterior Peroneus Longus Peroneus Brevis Intrinsic Muscles Lumbricales Plantarflexory force across MPJ/Proximal phalanx Quadratus Plantae Interossei Plantarflexory force across MPJ, stabilization in transverse plane Extensor Digitorum Brevis Flexor Digitorum Brevis Muscles Involved
Gait Patterns • Flexor Stabilization • Most common, FDL/FDB overpower the interossei • Flexor Substitution • Caused by weak Tendo-Achilles where PB, PL, TP, FDL, FHL try to make up for the weak calf muscles and again overpower the interossei • Extensor Substitution • EDL overpowers the lumbricales, usually seen in high arched foot and/or ankle equinus
How do we Treat Crooked Toes? • We can try to accommodate the hammertoes with non-surgical treatment such as: • Orthotics • Metatarsal pads • Soft toe caps • Wide, Extra-depth shoes • Digital spacers • Taping/Splinting • Crest Pads
When non-surgical methods fail, we start thinking about surgical options.We need to decide what techniques and products work best for our patients.So what’s out there…
Smooth K-Wire • Advantages: • Quick application • Cheap • Able to cross the MPJ if needed • Disadvantages: • Pin is sticking out of toe and can catch on things • No compression • Increased risk of infection • Toe can rotate • Wire can bend
Screw Fixation • Advantages: • Not sticking out of skin • Provides compression • Disadvantages: • Toe is completely straight and can’t bend at DIPJ • Can still rotate • More difficult to remove than a wire if needed
Absorbable Pins • Advantages: • Internal • Cost efficient • Disadvantages: • No compression • Toe can rotate • Patient can have a reaction to the material
Stay Fuse • Advantages: • Internal • Provide some compression • Different sizes • Disadvantages: • 2 pieces • Costly • Higher chance for error
Biomet Weil-Carver Implant • Advantages: • Resorbable with Lactosorb: poly-L-lactic/polyglycolic acid copolymer • Retains strength 6-8wks, degrades approx 12 mos • Partially threaded, barbed to prevent pistoning • Disadvantages: • Toe can still rotate • Doesn’t provide complete compression
Smart Toe • Advantages: • Internal • Provides some compression • Prevents rotation • Also comes with an angled version • Disadvantages: • Must be cooled prior to implantation • Costly
X Fuse • Advantages and Disadvantages comparable to the Smart Toe
Orthopro I Fuse • New product in development • Comes in Screw-Barb and Barb-Barb configurations • Small and Large sizes • Also comes either angled at 10 degrees or straight
Summary • As reps you have more influence on doctors than you know. However: • Once you can get surgeons to break out of their “old habits” they will: • 1. Use the quickest implant to insert. • 2. The implant that has minimal complications, high fusion rate and high patient satisfaction. • Note: In my opinion, the best implant as far as a rep is concerned is one that has a high degree of “dummy factor”. If the implant is easy to put in: ie. Doesn’t require dry ice etc. then the rep doesn’t have to be present for every case. (Earning income while golfing)