Download
1 / 89
910 likes | 984 Views
PITUITARY TUMORS. PITUITARY TUMORS. Account for 10-25 % of brain tumors Medium age at debut: between 20-50 years Children rarely have pituitary adenomas. Most tumor in children are craniphariogiomas and are associated with growth failure and diabetes insipidus.

E N D
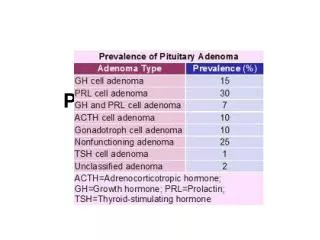
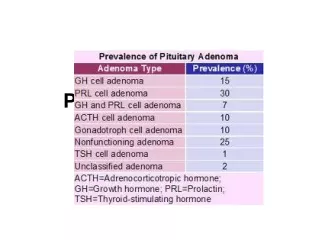
PITUITARY TUMORS • Account for 10-25 % of brain tumors • Medium age at debut: between 20-50 years • Children rarely have pituitary adenomas. Most tumor in children are craniphariogiomas and are associated with growth failure and diabetes insipidus. • Most pituitary adenomas in children are prolactinomas • Prolactinomas, Gh secreting adenomas and ACTH-secreting adenomas are more frequent in women. GH secreting adenomas are more frequent in men.
PITUITARY TUMORS - CLASSIFICATION According to their size: • Microadenomas:have less than 1 cm, do not modify the shape of sella turcica and do not produce pituitary tumor syndrome • Macroadenomas:have nore tahn 1 cm. and according to the direction they develop produce “the syndrome of pituitary tumors” According to their degree of aggression • Benign adenomas • Invasive adenomas • Carcinamas: less then 1 % of pituitary tumors
HISTOGENESISOF PITUITARY TUMORS Two hit hypothesis: Pituitary adenomas are monoclonal tumors Polyclonal adenomas may result from excessive stimulation of pituitary by specific releasing hormones Pituitary cells have a genetic protective factor against tumor proliferation. Lost of one protective allelle - first hit is not associated with tumor transformation, a point mutation of the second allelle – second hit results in tumor proliferation . Tumor occurs only if both protective factors are lost
HISTOGENESISOF PITUITARY TUMORS Anotherpathogenic hypothesis is an activating mutation of alpha subunit of GTP-binding protein which activates cAMP and stimulates cell proliferation În MEN 1– Multiple Endocrine Neoplasia type 1 there is an autosomal dominant deletion of a protective gene MENINE encoded on chromosome 11 (11q13)and multiple tumors simultaneous or successive occur: - multiple parathyroid adenoams with primary hyperparathyroidism - gastro-entero-pancreatic tumors: gastrinoma, insulinoma, glucagonoma - carcinoid tumors - adrenal adenomas - lipomas - facial angiofibromas
PITUITARY TUMOR SYNDROME • NEUROLOGIC SYMPTOMS: • Headache • Nerves III, IV and VI which cross the cavernous sinus • Temporal seizures • Other seizures • Meningeal signs • OPHTALMOLOGICSIGNS • Decreased visual acuity • Reduction of visual field according to tumor extension • Exophtalmos : rare • RADIOLOGICAL SYGNS • Enlarged surface of sella turcica • Radiologic signs specific for some pituitary adenomas: acromegaly
Effects of pituitary enlargement on optic chiasma and visual field
Loss of lateral visual field due to optic chiasm compression
Radiological signs in pituitary macroadenoma: enlarged sella turcica, destroyed sellar walls
DIAGNOSIS OF PITUITARY ADENOMAS • Clinical suspicion • Assessment of pituitary hormones to determine hormonal secretion of adenomas and level of other pituitary hormones in case if pituitary is partially dystroyed. • Radiograph of sella turcica: useful in case of macroadenomas • CT orMRI of hypothalamic-pituitary area • Inhibitory tests, biochemical markers for some adenomas
TREATMENT of PITUITARY ADENOMAS • SURGERY • RADIOTHERAPY • PHARMACOTHERAPY
SURGICAL TREATMENT OF PITUITARY ADENOMAS • First intention therapy for all adenomas with exception of those which have a proven beneficial pharmacological treatment • Immediately indicated in tumors which exert compression over structures from the proximity and involve a risk for sight loss or have intracranial hypertension. • Is an emergency treatment for pituitary apoplexy – pituitary infarct. • May be delayed until pharmacological treatment may reduce tumor volume and make the tumor more accessible to surgery in some responsive cases
SURGICAL TREATMENT OF PITUITARY ADENOMAS Aim of surgery: • To reduce mass effect produced by large tumors over adiacent structures • To inhibit hormone secretion in pituitary secreting adenomas • To preserve morphologic and functional integrity of the pituitary
SURGICAL TREATMENT OF PITUITARY ADENOMAS Approach of the pituitary during surgery: • Transcranial approach: in large tumors with extra selar extension. The aim is to reduce tumor volume and has greater number of complications • Transphenoidal approach – is used in most adenomas with medium and small size. This treatment have no complications in a skillful hand and preserves the pituitary function if it was not previously affected. • Complete cured: 90 % of microadenomas • Tumor reduction without complete cure in larger tumors
SURGICAL TREATMENT OF PITUITARY ADENOMAS Complication of pituitary surgery depend of the size of the tumor and quality of surgery: • Death by carotid injury • Severe complication due to injury of cavernosal sinus and nerves III,IV and VI • Brain injuries • Chiasma injury with complete sight loss • Infections: meningitis, enchephalitis • Cerebro-spinal flud fistula • Diabetes insipidus: permanent 5 % of (frequently transitory condition – some weeks) • Syndrome of inapropriate vasopressine secretion 10 % • Hypopituitarism 5-10 % in large tumors
IRRADIATION IN PITUITARY ADENOMAS Convenţional irradiation: The tumor is irradiated based on a computerized program which includes CT and MRI in order to spare the proximal regions with CT/IRM 4000 – 5000 cGy, in fractionated doses of 180 – 200 cGy per day, 5 days per week Succes: • 80 % in acromegaly, but full effect appear variably in time until 8 years and even more • 55 – 60 % in ACTH-secreting tumors , in a shorter time • In prolactinomas the response rate is less important because tumor secretion may be successfully controlled with dopamine agonists
IRRADIATION IN PITUITARY ADENOMAS Complications of conventional irradiation: • Hypopituitarism in 50-60 % of cases in 8-10 years • Optic nerve injury • Brain radio necrosis • Occurrence of other neoplasia of the brain favor by previous irradiation Gamma knife delivers in one MRI –guided the entire dose of irradiation on a very small field The effects of irradiation are more rapid – until 4 years Only in tumors which are more distant of the optic chiasm: at least 4 mm. Until the cure obtained by irradiation the tumor secretion and growth must be controlled by pharmacotherapy
Prolactinomas and hyperprolactinemia Prolactin excess inhibits gonadotropins secretion In women: • Secondary amenorrhea, oligomenorrhea, infertility • Galactorhea • Hirsutism • Signs of estrogen deficiency with genital atrophy • Osteoporosis • Pituitary failure in large prolactinomas Most prolactinomas in women are microadenomas.
Prolactinomas and hyperprolactinemia In men: decreased testosterone secretion with: • Decreased libido • Erectile dysfunction • Infertility • rare: gynecomastia şi galactorhea • Pituitary failure In men most prolactinomas are macroprolactinomas and are associated with “pituitary tumor syndrome”
Microprolactinoma Macroprolactinoma
OTHER CAUSES OF HYPERPROLACTINEMIA • Physiological: breast feeding, sexual activity, sleep, stimulation of mamary gland • Interruption of conection between hypothalamus and pituitary and inhibitory control of the hypothalamus over pituitary, stalk section, stalk compression by other tumors, hypothalamic tumors • Empty sella syndrome • Drugs which inhibit dopamine: psychotropes, antidepressives, l-DOPA, 5HT2 inhibitors, estrogeni, oral contraceptives • Hypothalamic diseases: sarcoidosis, hysticytosis • Polycystic ovarian disease, acromegaly, hipothyroidism, kidney failure, liver cirrhosis • Torax unjuries
ASSESSEMENT OH HYPERPROLACTINEMIA • Prolactin values • Prolactin levels correlates with tumor size • Normal prolactin levels: 9-25 ng/ ml • 50 ng/ ml functional hyperprolactinemia • between 50-100 ng/ ml microprolactinomas • over 100 ng/ ml macroprolactinomas • Bromocriptine test: • 2,5 mg bromocriptinemust reduce prolactin levels • Assessement of lesions: CT, IRM
TREATMENT OF PROLACTINOMAS Pharmacotherapy – dopamine agonists • First choice treatment in microprolactinomas and pre treatment in macroprolactinomas in order to reduce tumor size and facilitate surgery • Bromocriptine: 2,5 – 20 mg /day • Cabergolină: 0,5 – 3,5 mg /week • quinagolid • Effects of pharmacotherapy: - menses occur again - fertility is restored - during pregnancy the treatment may be stoped - during pregnancy the tumor is followed by assessing the visual field
TREATMENT OF PROLACTINOMAS SSurgery • For large tumors with compressive symptoms • May be done after previous pharmacotherapy • Effects of surgery: - in best cases gonadotropin secretion occurs again - risks and complications are similar to other pituitary tumors submited to surgery - residual disease may be controlled with dopamine agonists C. External irradiation is rarely needed
ACROMEGALY PREVALENCE: • 40 – 60 cases / 1 milion /year • 3-2 new cases per year • 1 / 15.000 person
ACROMEGALY Causes : • sporadic: • Adenoama pure high granulated, sparse granulate • Mixed GH and prolactin secreting adenomas • Acidofilic adenoams with stem cells • Ectopic adenomas • GH secreting carcinoma • Mc Cune-Albright syndrome • Familial forms: izolated, MEN 1, Carney complex, FIPA - • Hypothalamic GH.RH excess: harmartoms, gangliocytoma, glyoma, • Extrahypothalamic GH-RH secretion • Pancreatic carcinoids, bronchial carcinoma MTC,
Development of the disease is insidious and graduated during years, the disease being recognized 10 years after real debut
Acromegaly – signs and symptoms • Signs and symptoms of the disease are determined by the effects of GH and IGF1 over target tissues after the epiphyseal growth plates are closed. In case of a precocious debut gigantism occurs • Short and flat bones are more affected, • GH and IGF1 excess produce • Hypertrophy of all structures containig connective tissue and bone • Metabolic abnormalities