Download
1 / 57
580 likes | 781 Views
Spongiform Encephalopathies. Dr. Cathal Collins 14/02/05. Introduction. Prion disease Neurodegenerative Long incubation period Progresses inexorably 5 human prion diseases: Kuru Creutzfeldt-Jokob disease (CJD) New variant CJD Gerstmann-Straussler-Scheinker syndrome

E N D
Spongiform Encephalopathies Dr. Cathal Collins 14/02/05
Introduction • Prion disease • Neurodegenerative • Long incubation period • Progresses inexorably • 5 human prion diseases: • Kuru • Creutzfeldt-Jokob disease (CJD) • New variant CJD • Gerstmann-Straussler-Scheinker syndrome • Fatal familial insomnia
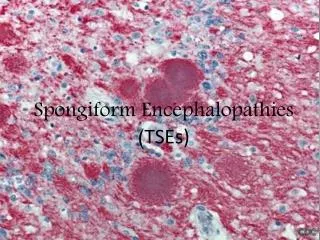
Neuropathology • Neuronal loss • Proliferation of glial cells • Absence of an inflammatory response • Presence of small vacuoles which produces a spongiform appearance
Animal prion diseases • Scrapie: sheep, goats; first described 1738 • Transmissible Mink Encephalopathy: minks; 1964 • Chronic Wasting Disease: mule, deer, elk; 1980 • Bovine Spongiform Encephalopathy: cattle; 1986 • Feline Spongiform Encephalopathy: cats; 1990
BSE History in UK • 1985: first cases of BSE • 1988: June BSE made notifiable July Ruminant feed banned August Compulsory slaughter and destruction of suspect cattle • 1989 February Southwood report November Ban of sale of bovine offal for human consumption
BSE History in UK • 1990 November Bovine offal feed ban for all animals and birds • 1992: Peak incidence of BSE • 1996: First cases of nvCJD Further restriction of bovine products from food and food chains
Dr. Stanley Prusiner: coined the term “prion” in 1982: proteinacious infectious particle Small infectious pathogen containing protein and lacking nucleic acid One characteristic feature is their resistance to a number of normal decontaminating procedures Resistant to: Aldehydes e.g formaldehydes Nucleases Heat (80C) UV and ionising radiation Non-ionic detergents Biology of Prions
Biology of Prions • Inacticated by: • Prolonged autoclaving (at 121C and 15psi for 4.5h) • Immersion in 1M NaOH (for 30 min, repeat 3 times) • Immersion in strong organic solvents • Inadequate autoclaving can establish heat resistant subpopulations • Stainless steel instruments may also retain infectivity even after treatment with 10% formaldehyde
Prion Protein (PrP) • The gene (PRPN) is located on the short arm of chromosome 20 • Encodes a protein (PrPc) found in normal brain (alpha helical); normal function unknown • PrPsc (PrP in scrapie infected anmals) is a conformational isomer of PrPc (B-pleated sheet) • PrPsc is resistant to digestion with proteases and has a tendency to polymerise into scrapie-associated fibrils or prion rods
Biosynthesis of PrPc • Key step is modification of amino and carboxy terminals with the addition of a phosphatidylinositol glycolipid which serves to anchor the protein to the cell surface • PrPc is found attached to plasma membranes of neurons and may be concentrated at synaptic membranes • PrPc has transmembranous domains • Degraded after endocytosis in acidic vesicles
PrPsc • Accumulates within cells; does not normally appear on the cell surface • Found predominantly in cytoplasmic vacuoles and secondary lysosomes • Studies with mice either devoid of PrPc or with abnormal isoforms indicate that host PrPc must be present for the development of prion disease • Prion diseases result from accumulation of abnormal isoforms of the PrP which is dependent upon conversion of PrPc to PrPsc
PrPsc • How the first molecule of PrPsc appears in the host remains a mystery • Exogenous source in sporadic and iatrogenic CJD • Mutation in PRNP gene in familial forms • The initial appearance (?de novo) probably triggers the replication of PrPsc; PrPc acts as a nidus for the formation of PrPsc on challenge
PrPsc • Prior to transport to the nervous system, follicular dendritic cells within germinal centres of lymhoid tissue appear to act as a reservoir for the protein • Two reports suggest that complement plays a role in early pathogenesis ( C3, C1q, Bf/C2, or complement receptors) • Transport of PrPsc to the nervous system occurs via axons
Neurotoxicity of prion protein • PrPsc causes apoptosis and cell death • Misfolded PrP is transported to the cytosol for degradation- even small amounts of this protein in the cytosol are highly neurotoxic • Accumulation of this protein may be an important step in prion disease pathogenesis
Genetics • PRNP encodes PrP and is located on the short arm of chromosome 20 • A strong link has been established between mutations in the PRNP gene and forms of prion disease with a familial predisposition (fCJD, GSS, FFI) • More than 50 different mutations have been identified • A single mutation may produce different clinical phenotypes in different individuals or families
Genetics • The phenotype of a particular mutation may be influenced by the nature of the amino acids present at codon 129 • Normal individuals have either valine or methionine at this site • PRNP is an autosomal dominant gene; can be homozygous or heterozygous • D178N mutation (asparagine for aspartic acid in codon 178): Homozygous for valine at codon 129 appear to develop CJD; those homozygous for methionine tend to have FFI
Genetics: Codon 129 • Molecular classification scheme for sporadic CJD based upon codon 129 polymorphism and characterisation of the properties of PrPsc • A pattern of type 1 PrPsc plus at least 1 methionine at codon 129 was demonstrated in 70% • Type 2 PrPsc plus codon 129 homozygous or heterozygous for valine was present in 25% and associated with ataxia
Genetics: CJD • Familial CJD: most common mutation is a substitution of lysine for glutamine in codon 200; phenotype may depend on codon 129 • Sporadic CJD and iatrogenic CJD are not associated with PRNP gene mutations; however in these forms and nvCJD, phenotyping at codon 129 appears to affect susceptibility and perhaps expression of the clinical illness
Genetics: GSS and FFI • GSS - P102L mutation is the most common PRNP - large degree of phenotypic heterogeneity - polymorphism at codon 129 may play a modulating role • FFI -D178N mutation predominant in those homozygous for methionine at codon 129
Kuru • First transmissible neurodegenerative disease to be identified and well studied • Has served as the prototype of human prion diseases
Kuru- Epidemiology • Was endemic in Papua New Guinea among the Fore tribes • Felt to be transmitted from person to person by ritual cannibalism • Still remains uncertain as to whether the brain was actually eaten, but it was handled after death, particularly by females and children • No cases observed since these practices discontinued • Primary cause of death in the tribes in 1960s
Kuru- Clinical Features • Ambulatory phase: tremors (kuru=shivering), ataxia and postural instability • Sedentary stage: loss of ambulation resulting from increased tremors and ataxia; involuntary movements • Late stage: dementia, indifference • Terminal stage: frontal release signs, cerebellar type dysarthria and inability to get out of bed • Death typically due to pneumonia occurring within 9-24 months form onset of disease
Kuru- Diagnosis&Pathology • CSF unremarkable, EEG not characteristic • Pathological hallmark is PrPsc-reactive plaques occurring with the greatest frequency in the cerebellum; neuronal loss and hypertrophy of astrocytes is also observed
Creutzfeld-Jakob Disease • Most frequent of the human prion diseases • Still very rare • Sporadic (sCJD), familial (fCJD), iatrogenic (iCJD) and new variant (nvCJD)
CJD- Epidemiology • Approx 1 case per 1 million population/year • World-wide distribution • Mean age of onset is 57-62 • Patients with nvCJD and iCJD tend to be much younger • No gender predilection • Incidence increased 30-100 fold in certain areas of North Africa, Israel and Slovakia, due primarily to clusters of fCJD • Vast majoriy sporadic (85-95%), 5-15% fCJD, <5% iCJD
Iatrogenic CJD • Following administration of cadaveric human pituitary hormones, dural grafttransplants, use of dural mater in radiographic embolisation procedures, corneal transplants, liver transplants, and the use of contaminated neurosurgical instruments or stereotactic depth electrodes • Hx of preceding infusion does not increase risk of developing CJD (epidemiology studies); however low levels of infectivity in in vitro studies
CJD- Clinical Features • Rapidly progressive mental deterioration and myoclonus are two cardinal manifestations of sCJD • Number of variants or subtypes of disease based based upon area of involvement of the brain • Visual • Cerebellar • Thalamic • Striatal • Variants of sCJD also classified based on genotype of PRNP and the molecular properties of the pathological PrPsc
CJD- Clinical Features • Mental deterioration may manifest as dementia, behavioural abnormalities and deficits involving higher cortical function • Concentration, memory and judgement difficulties are frequent early signs • Mood changes such as apathy and depression are common • Dementia becomes dominant and can advance rapidly • Death usually occurs within one year
CJD- Clinical Features • Myoclonus, especially provoked by startle, is present in more than 90% • sCJD should always be considered in a patient with a combination of a rapidly progressive dementia and myoclonus • Extrapyramidal signs such as hypokinesia and cerebellar manifestations including nystagmus and ataxia occur in 2/3 • Corticospinal tract involvement in 40-80% • Sensory signs and symptoms are common in nvCJD; otherwise extremely atypical
Subtypes of sCJD • Clinical phenotypes of sCJD associated with molecular subtypes determined by the PRNP gene codon 129 genotype and the pathologic prion protein (PrPsc) type • PRNP genotype homozygous or heterozygous for methionine (M) or valine (V) at codon 129 • The PrPsc type is determined by Western blot analysis amd classified in the Parchi/Gambetti nomenclature as type 1 or type 2 • Alternate Collinge nomenclature distinguishes 4 PrPsc subtypes: types 1 and 2 correspond with P&G PrPsc 1; 3 and 4 with P&G PrPsc 2
Subtypes of sCJD • 6 clinical phenotypes of sCJD • MM1 and MV1 (myoclonic, Heidenhain variant) account for about 70% of cases and correlate with the “classic CJD” phenotype • VV2 (ataxic variant) accounts for 16% • MV2 (Kuru plaque variant): 9% • MM2 thalamic, MM2 cortical and VV1 account for the rest
CJD- Diagnosis • Clinical and laboratory features generally are sufficient for a ‘probable’ diagnosis of sCJD • WHO criteria for ‘probable’ diagnosis: • Progressive dementia • >/=2 of 4 of: myoclonus; visual or cerebellar disturbance; pyramidal/extrapyramidal dysfunction; akinetic mutism • A typical EEG during an illness of any duration and/or positive 14-3-3 CSF assay with a clinical duration to death in less than 2 years • Routine investigations should not suggest an alternative diagnosis
CJD-Diagnosis • A definitive diagnosis requires these features in combination with one or more of the following: • Loss of neurons, gliosis, spongiform degeneration, or plaqes postive for PrPsc on histopathlogy of brain tissue • Positive PrPsc staining following pretreatment of brain tissue to destroy PrPc reactivity • Positive histoblotting of brain tissue extracts for PrPsc after treatment to destroy PrPc reactivity • Transmission of characteristc neurodegenerative disease to experimental animals • Demonstration of PRNP gene mutations
CJD- Diagnosis • Neuroimaging: diffusion weighted MRI- can detect abnormalities as early as 3 weeks of symptom duration, CT generally normal • EEG: aids diagnosis: characteristic pattern of periodic synchronous bi or triphasic sharp wave complexes (PSWCs) • Protein markers: 14-3-3 protein in CSF- especially in those with classical subtypes of sCJD • Pathological studies of brain material to detect protease resistant PrPsc remains gold standard
New Variant CJD • Initial reports of nvCJD in 1996 quickly focused intense interest on the human prion diseases • Linked with bovine spongiform encephalopathy • Unique epidemiological features of this illness led to early recognition that this was indeed a ”new variant”
nvCJD- Epidemiology • First report of a case of nvCJD in a 16 year old from the UK appeared in 1995 was quickly followed in 1996 by 22 other cases • All bar one of the initial cases were from the UK • January 2004- 155 cases world-wide • 145 from UK, 6 from France, 1 each from Ireland, Italy, Canada and the US • All except the italian had resided in countries with known BSE
nvCJD V sCJD • nvCJD is distinguished from sCJD by • A considerably younger age of onset (mean age of onset 29 versus 65) • Less rapid progression of disease (duration 14 months versus 4-5) • Differences in clinical presentation (sensory and psychiatric symptoms prominent in nvCJD) • Type 2 (P&G)/ type 4 (Collinge) PrPsc in nvCJD • Differences in neuropathology
nvCJD- Clinical features • 63/100 of the 1st cases presented initially with psychiatric symptoms • Neurological symptoms preceded psychiatric in 15 • Both were present in 22 • Psychiatric symptoms include depression, apathy, anxiety, psychosis and intermittent delusions • Sensory abnoramalities include dysaesthesias and paraesthesia of the face, hands, feet, legs or even hemibody
nvCJD- Clinical features • Once neurological symptoms, typically ataxia, becomes evident, progression is more rapid • Cognitive impairment, involuntary movements, immobility, unresponsiveness, and mutism are common signs as the disease progresses • Paresis of upward gaze may be present (uncommon in other forms of CJD)
nvCJD- Diagnosis • CSF studies rarely helpful: 14-3-3 is not a sensitive marker • Combination of 14-3-3 and tau protein in CSF may be useful • MRI better than CT: MRI may show signal hyperintensity in the pulvinar (pulvinar sign) or in both pulvinar and dorsomedial thalamus (hockey stick sign) • EEG: abnormal in 70% but only slow wave pattern
nvCJD- Diagnosis • PRNP gene mutations are not present in nvCJD, but all patients with clinically expressed nvCJD have been homozygous for methionine at codon 129 • Type 2 PrPsc (P&G nomenclature) or type 4 PrPsc in the Collinge nomenclature has been found in patients with nvCJD (not characteristic of other human prion diseases)
nvCJD- Neuropathology • A number of neuropathological feature distinguish nvCJD from sCJD: • Presence of plaques, which stain intensely for PrPsc, distributed throughout the cerebrum and cerebellum and to a lesser extent the basal ganglia and thalamus • The plaques have an eosinophilic centre and pale periphery with surrounding spongiform changes • Cases of kuru and GSS have similar but not identical plaques • The cerebellum is characteristically involved in nvCJD • nvCJD has distinct type 4 PrPsc
nvCJD- Links • 2 cases of possible transfusion transmisssion of nvCJD have been reported • There is increasing evidence supporting the possibility that nvCJD represents bovine-to-human transmission of BSE
nvCJD and BSE • The appearance of nvCJD followed an epidemic of BSE in the UK • The removal of organic solvents, which inactivate PrPsc, from the rendering process for bovine offal and the subsequent use of the offal as a component of feed for cattle has been suggested as a mechanism for amplifying the epidemic in animals • Approx 50,000 infected cattle are estimated to have entered the food chain
nvCJD and BSE • The prohibition of ruminant-derived proteins in feeds for all animals and poultry in november 1990 and the banning of consumption of animals over the age of 30 months in March 1996 has led to a dramatic decline in cases of BSE • Evidence in the favour of the association between nvCJD and BSE includes the type 4 pattern of PrPsc which has not been seen in other prion diseases
nvCJD and BSE • Despite the apparent link between nvCJD and BSE, the number of cases of nvCJD has remained small. Possible reasons include: • Low levels of PrPsc in milk and meat • Inefficiency of oral route of infection • Restriction of spread based upon a species barrier • Low incidence of host genetic factors such as the frequency of homozygosity at codon 129