Download

1 / 50
560 likes | 959 Views
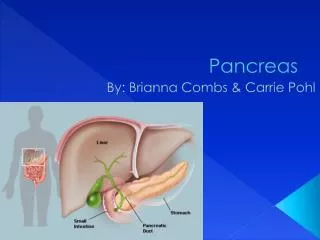
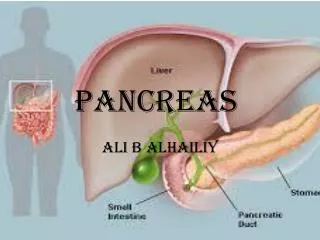
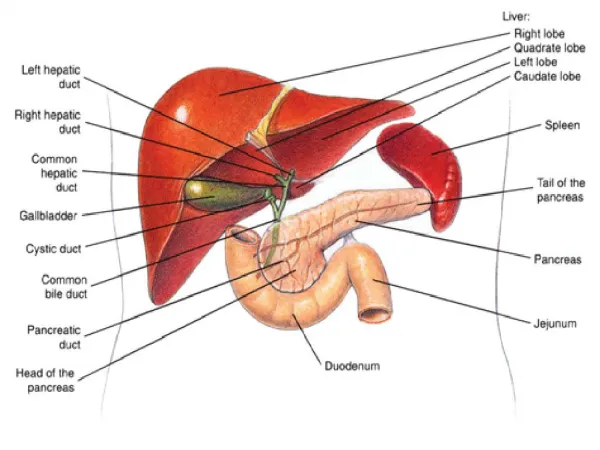
Pancreas. Tail. Body. Head. Neck. Uncinate process. Pancreas. Exocrine Acinar cells Spontaneous secretion is minimal Secretin – evokes bicarbonate-rich fluid secretion Cholecystokinin (pancreozymin) – evokes pancreatic enzymes secretion Endocrine Islet cells B cells – insulin

E N D
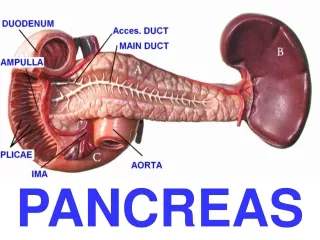
Tail Body Head Neck Uncinate process
Pancreas • Exocrine • Acinar cells • Spontaneous secretion is minimal • Secretin – evokes bicarbonate-rich fluid secretion • Cholecystokinin (pancreozymin) – evokes pancreatic enzymes secretion • Endocrine • Islet cells • B cells – insulin • A cells – glucagon • D cells – somatostatin • Pancreatic polypeptide cells
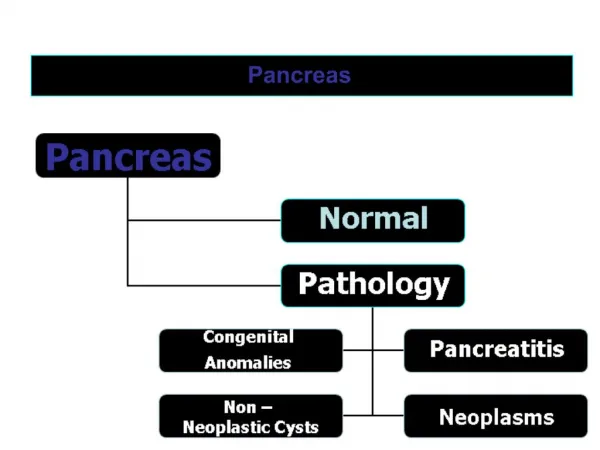
Pancreatitis • Acute pancreatitis • Mild • Severe • Chronic pancreatitis
Atlanta Definitions • Acute Pancreatitis • Acute inflammatory process of the pancreas, with variable involvement of other regional tissues or remote organs systems • Mild Acute Pancreatitis • Pancreatitis associate with minimal organ dysfunction and an uneventful recovery. The predominant feature is interstitial oedema of the gland • Severe Acute Pancreatitis • It is associate with organ failure and /or local complication such as necrosis ( with infection) pseudocyst or abscess. Most often this is an expression of the development of pancreatic necrosis although patients with oedematous pancreatitis may manifest clinical features of severe attack
Etiology Gallstones ETOH Iatrogenic ERCP Drugs Steroid, furosemide, thiazide diuretics, azathioprine Infection Cytomegalovirus, ascariasis, scropion venom, mumps, viral hepatitis Trauma Anatomical anomalies Pancreatic Divisum Genetic Familial pancreatitis Cystic fibrosis Alpha-antitrypsin deficiency (risk for ca pancreas) Acute pancreatitis
Pancreatic Divisum • Malunion of the pancreatic ducts from the ventral and dorsal buds of the pancreas…. Results in complete or partial separation of the duct systems of Wirsung (main – dorsal) and Santorini (accessory – ventral) • 0.3 – 5.8% endoscopy series • 5 - 14% autopsy studies • Prone to pancreatitis due to poor outflow of the accessory duct system • But majority of the patients with pancreatic divisum don’t have any association with acute pancreatitsi
Pathogenesis – molecular biology • Premature activation: intracellular zymogens • Nuclear factor (Kappa) B • Activator Protein 1 • Cytokines, Chemokines • Pathological Calcium influx • Gap junction disruption – ETOH • Neurally mediated inflammation • Substance P
Acute pancreatitis • Symptoms • Acute Vs Chronic • History / X ray / CT scans / Pancreatic duct assessment (ERCP / MRCP) • Etiology factors • Complications • MOF / ARDS / SIRS → ICU • Infective necrosis → Operation • Pseudocyst • Splenic vein / portal vein thrombosis → varices / cirrhosis • Endocrine insufficiency DM, absorption • Chronic pancreatitis • Ductal strictures • Pancreatic Malignant Neoplasm • Cardio / Respiratory / Renal / Vascular complications
Acute pancreatitis • Rapid progressive onset of pain • Upper abdominal pain -T G R, may mimic any acute abdominal conditions • AXR -sentinel loop, calcification, gallstones • CXR – right pleural effusion (reactive sympathetic effusion) 20% • Cullen sign (Thomas Stephen Cullen – Prof of Gynaecology. John Hopkins Uni) • Grey turner sign (George Grey Turner – Prof of Surgery. London) • Amylase • Lipase
Multifactorial Scoring System • To predict the prognosis • Positive predictive value 50% • Ranson’s • Glasgow • Apache II • 12 routinely measured physiological and biochemical parameters, couple with a score for age and pre-existing health status
Biliary Age >70BUN >0.7 WCC >16 HCT↓10% Glucose >12 Ca <2.0 LDH >400BE <-5 AST >250 Oxygen < 60mmHg Fluid >6 liters Non biliary Age >55 BUN >1.8 WCC >16 HCT ↓ 10% Glucose >11 Ca <2.0 LDH >350 BE <-4 AST >250 Oxygen <60mmHg Fluid >6 liters Ranson’s Criteria
Age >55 WCC > 15 Urea > 16 PaO2 < 60mmHg Glucose >10 LDH > 600 AST / ALT > 600 Ca < 2 Albumin < 22 Glasgow Score
Assessment • Apache II scoring system • >9 severe attack • >6, 95% will have complications • C-reactive protein • 36 hours after onset of illness • >210 mgI-1 first 4 days • >120 mgI-1 at end of first week • CT severity index / MRI • MOF
MOF • Respiratory • Neurocerebral • Cardiovascular • Haematological • Renal • Hepatobiliary / Gastointestinal Bernard MOF scoring system: This scoring system does not include hepatic index
Etiology factor Early ERCP Supportive Organs specific Ventilation / haemofiltration / inotropes Early Intensive support Nutrition – early jejunal feeding / TPN Octreotide / Somatostatin Anticytokines therapy / Anti-inflammatory agents Gut selective Decontamination – prevent translocation of bacteria : SIRS Management of Complications: Antibiotic Surgery – infective necrosis Radiological guided drainage – intraperitoneal abscess /collection Management
Nutrition • Enteral feeding • Jejunostomy feeding • Nutritional support • Prevent translocation of GI bacteria • TPN • Only if gut not usable
SurgeryIndications • Infective necrosis • Clinical / microbiological confirmation • Uncontrolled sepsis • Secondary complications • Pseudoaneurysm • Intestinal obstruction • Perforation of bowel (ERCP) • Cholecystectomy • Late complications consider surgery when applicable • Pseudocyst • Pancreatic duct stricture / stenosis • Pancreatic ductal stones
Chronic Pancreatitis • Continuing inflammatory disease of the pancreas characterized by irreversible morphological change typically causing pain and / or permanent loss of pancreatic function
Chronic Pancreatitis - diagnosis X Rays CT- sensitivity 75-90%; specificity 85-100% (pancreatic calcification) degree of calcification does not correlate with the degree of exocrine insufficiency MRCP, ERCP MRI • History / Examination • Radiological • Histopathological • Functional deficits • Histopathological changes: • Parenchymal fibrosis, ductal stricture, atrophy of acinar and islet cells • Calcific pancreatitis - alcohol • fibrosis, calcification, and protein plugging • Obstructive Pancreatitis - stones/Carcinoma • dilatation, acinar atrophy and fibrosis • Inflammatory Pancreatitis • autoimmune disease (Idopahtic, Sjogren syndrome & Sclerosing Cholangitis) • Malabsorption • DM • Sudan staining of stool • 72hrs stool collection with diet containing 100g fat per day, if more than 7g per day excretion is abnormal • Faecal trypsin / chymotrypsin • Lundh test – direct duodenal aspiration • Secretin-pancreozymin test • Bentiromide test - Enzyme reaction
Chronic PancreatitisSeverity • No agreeable assessment method to determine the severity of chronic pancreatitis • Based on the level of pancreatic dysfunction and symptoms • Again clinical history and assessment • Radiological assessment for any ductal disruption
Chronic Pancreatitis • Cambridge Classification • According to ductal anomaly
Chronic Pancreatitis: etiology • ETOH 70% • Anatomical – pancreatic divisum, ductal stricture • Genetic – cystic fibrosis, antitrypsin deficiency • Hypercalcaemia • Tropical pancreatitis • Nutritional pancreatitis • Idiopathic Chronic Pancreatitis • Early onset <35 yo – poor prognosis • Late onset >45 yo • Decrease HCO3 and increase protein production, increase viscosity lead to stone formation • Acinar cell damage • Repeat attack lead to fat necrosis, with interlobular fibrosis • Liver impairment lead to failure to detoxify toxic substance causing direct damage to the pancreas
Chronic Pancreatitis • Clinical features: • Multiple somatic / psychosocial symptoms • Endocrine / exocrine dysfunction • Burn out syndrome • Usually 15-20 years after onset of illness • Malignancy
Chronic PancreatitisManagement • Manage symptoms • Pain control – med / thoracoscopic splanchniectomy • Psychosocial support • ETOH • Endocrine / exocrine function • Pancreatic enzyme replacement : PPI • DM control • Malnutrition • Malignancy - investigate if indicated
Chronic Pancreatitis • Other complicatons • Pseudocyst • Splenic vein thrombosis • Hypersplenism / GIB – require splenectomy • Mesenteric / Portal vein thrombosis • Pancreatic ductal deformity / stones • Pancreatic ascites / pleural effusion
Chronic PancreatitisSurgery Indications • For focal disease / ductal anomaly • Bypass: pancreaticojejunostomy (Puestow procedure) duct >7mm • Distal Pancreatectomy • Whipple procedure • For pain • Thoracoscopic splanchniectomy • Frey’s operation – Bypass with resection of pancreatic head • If head is > 3cm in size • Bypass surgery – eg Puestow procedure • For suspected malignancy • Laparoscopy • Laparotomy Whipple Distal Pancreatectomy
Conservative Symptoms Malnutrition Endocrine dysfunction Education Psychosocial support ETOH Depression Invasive procedure ERCP Surgery Malignancy Chronic PancreatitisManagement
Pseudocyst • Collection of pancreatic juice enclosed in a wall of fibrous or granulation tissue that arises following an attack of severe pancreatitis. • Acute fluid collection: • Early in the course of acute pancreatitis and is located in or near the pancreas. The wall is ill defined. • Pancreatic cystic neoplasm: • Cystic lesion lined by epithelium, can be either benign or malignant in nature
Pseudocyst • 4 to 5 weeks after onset of acute pancreatitis • 40-60% Spontaneous resolution 6 weeks • > 6 weeks, risk of complication increase • Intervention • Surgical drainage – Open / Laparoscopic • Endoscopic drainage
Pseudocyst • Adequate assessment of pancreatic duct • Stricture / stones / morphology • Communication with cyst • Position of cyst in relation to other organs Cystojejunostomy Stomach Cystogastrostomy Stenting if communicate with PD
Psuedocyst • Complications • Bleeding • Abscess • Suspect Malignancy if atypical history or morphology • Suspect malignancy if • Septum / complex architecture • Solid component • Invasion of surrounding structures / metastatic lesion • Raised tumor marker • Lack of amylase in fluid aspirated from the cyst • Other solid lesions in pancreas • No previous history of pancreatitis / trauma Percutaneous Drainage
Weight loss 90% Pain 75% Malnutrition 75% Jaundice 70% Anorexia 60% Pruritus 40% Courvoisier’s sign 33% Diabetes mellitus 15% Ascites 5% GOO 5% Gastric outlet obstruction Pancreatic Carcinoma
Carcinoma of Pancreas Symptom and management depends on the location of the tumor Head of pancreas usually have better prognosis since their symptoms usually present earlier then tumor located at the body or tail of pancreas Usually asymptomatic until late in advance stage May present earlier with obstructive jaundice, duodenal ulceration etc…
Pancreatic Carcinoma • Etiology uncertain • Cigarette Smoking • Diabetes – long standing • Chronic pancreatitis - Amount of risk ? • Familial predispoistion 5-8% • Coffee / alcohol / organic solvents / petroleum
Ductal Epithelium Ductal cell AdenoCa Giant cell Ca Adenosquamous Ca Mucinous Ca MicroadenoCa Mucinous CystadenoCa Acinar cells Acinar cell Ca Acinar CystadenoCa Pancreatoblastoma Non Epithelial Tissue Fibrosarcoma Leiomyosarcoma Histocytoma Lymphoma Uncertain Histogenesis Papillary cystic neoplasm NeuroEndocrine tumors Hypervascular tumor Gastrinoma Insulinoma Vasoactive Intestinal Polypeptidoma Glucagonoma Pancreatic Neoplasms
Pancreatic carcinoma • Aim of management • Assess resectability • Curative Mx • Palliative Mx • Clinical & Radiological Staging • (i) Resectable • (ii) Non resectable • (iii) Metastatic disease • Absence of extrapancreatic disease • Absence of vascular involvement
Pancreatic carcinoma • Ultrasound abdomen • Double duct sign • CT abdomen & thorax • ERCP - 97% will have abnormality • Long irregular stricture • Double duct sign • Brush cytology only 40-50% positive • Endoscopic Ultrasonography • EUS - FNAC • Negative result does not rule out malignancy • Angiogram • When CT show possible vascular involvement in an otherwise resectable disease • Possible aberrant vascular anomaly
Pancreatic Carcinoma Type of surgery performed will depends on the location and involvement of the tumor • Whipple operation • Pylorus preserving Whipple • Gastric stasis in early post op period • Not for bulky tumor – inferior tumor clearance • Distal pancreatectomy +/- splenectomy
Pancreatic carcinoma • Palliative Mx – pain control • ChemoIrradiation • Biliary obstruction • Gastric outlet obstruction • Endoscopic stenting – plastic / metallic • Surgical bypass • Double bypass (gastric + biliary) • Gastric – gastrojejunostomy • Biliary – • Choledochojejunostomy • Choledochoduodenostomy
Pancreatic carcinoma • High index of clinical suspicion • Little clinical sign, non specific symptoms • Especially differentiating between pseudocyst and cystic neoplasm • History • Radiological features • Nature / Biochemistry of aspirated content • Amylase, tumor marker, cytology etc… • Tumor marker • CA 19.9 most specific, volume related • CA 125 • CEA