Download

1 / 20
240 likes | 881 Views
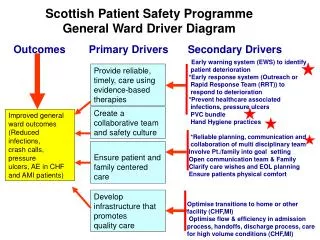
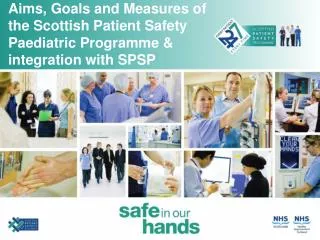
Scottish Patient Safety Paediatric Programme – Tests & Measures. Combined Child Services, NHS Grampian. Testing & Implementing Surgical Briefing Paediatric Trigger Tool PEWS PVC Bundle Medicines Reconciliation Safety Briefing Hand Hygiene SBAR. Measuring Surgical Briefing

E N D
Scottish Patient Safety Paediatric Programme – Tests & Measures Combined Child Services, NHS Grampian
Testing & Implementing Surgical Briefing Paediatric Trigger Tool PEWS PVC Bundle Medicines Reconciliation Safety Briefing Hand Hygiene SBAR Measuring Surgical Briefing Paediatric Trigger Tool PEWS PVC Bundle Medicines Reconciliation Safety Briefing Hand Hygiene Current Position
Paediatric Global Trigger Tool RACH Adverse Event Rate 2010 Team & Process • Identified core review group: Prof of surgery, Clinical Nurse Manager, Patient Safety Co-ordionator, Senior Charge Nurse. • Tested note review, amended form and re-tested. Training session provided by SPSP Programme Manager. • Note reviews now carried out monthly and reported internally and on Extranet. • Including all Paediatric admissions in our sample and not just those over 24hr stay. Learning so Far • Consensus between reviewers is very good. • Large number of the triggers relate to early warning data missing or incomplete. • Have feedback other learning points via the Clinical Teams who have taken action. Note reviews carried out 3 months later to ensure closed cases.
SBAR Change 1: Tested SBAR in HDU ward for communication between medical and nursing staff when telephoning. Posters Developed to facilitate education of staff on the tool. Change 2: Tested SBAR for transfer of patients from HDU to other wards. This facilitated HDU to begin their testingon handover back to the general wards. Change 3: HDU using SBAR to structure nursing handover and linked with safety briefing. Results have shown decreased handover time and improved communication. Change 4: SBAR implemented on surgical ward by Consultant as the method of communication re patient’s status, actions, treatment plan on the ward round. Staff view is that process is succinct. Change 5: NHSG Inter-hospital transfer SBAR is being adapted and tested to fit Child Health. Change 6: SBAR used by senior nurses in RACH as structure for formal reports.
Safety Brief Change 1: Adult pilot sites shared their safety briefing form and process with Child Health. V1 of form tested by SCN as part of handover in one team of medical ward. Changes made to process and form and continued testing and then implementing with one team. Change 2:Testing then spread to other medical team. Change 3: Implemented in medical ward on a daily basis. Learning shared with HDU. Change 4: Begun testing in HDU 1-3-5 all and now implemented. Change 5: Spread to other areas
Medicines ReconciliationExamples of tests/changes Change 1: V1 of form tested with 1 doctor, then tested with 1 nurse as either professional my collect medication details. Changes made to layout. Change 2:V2 including the introduction of insulin box tested 1,3 then required alterations highlighted Change 3: V3 tested also extensive discussion relating to children who have no regular medicines. To complete a form or not? Change 4: V4 created including a box to identify if the child is on no regular medicines. This is currently in use across PAU Change 5: V5 in progress need to reintroduce continue column in the reconciliation section. To be tested by Tuesday!
Medicines Data • Identification of sources is the only reason that not 100% • Clarity on sources • Feedback to individuals • Once 100% spread to rest of medical unit • Engagement of Surgical staff
Perioperative Change 1: Began testing the perioperative briefing, pause and debriefing process. Change 2:Tested posters to convey process for safety checks. Large surgical pause posters in each theatre to act as prompt for the process. Change 3: Checklist developed to capture data on briefing, pause and debrief. Tested and implemented. Change 4: Measuring compliance with the process from January 2010. Improvements noted in both briefing and pause compliance. Further work required on debriefing elements. Change 5: Now working on other perioperative measures.
Perioperative Data Next step to work on debriefing
PEWS Implementation Change 1: Document piloted and evaluated in A&E and Paediatric Assessment Unit (PAU). Found to conflict with Manchester Triage System. Change 2: Frequent education sessions for medical and nursing staff looking at evidence base and practical uses. Change 3: Implemented across RACH and Dr Gray’s Hospital Elgin. Change 4: Compliance monitoring commenced in the Surgical Unit. Change 5:Compliance monitoring now in PAU, Medical and Surgical Units.
PEWS Data and LearningMeasurement of Compliance Across 3 Areas
Next Steps For PEWS • Reprinting of PEWS charts to incorporate: - • Signature for ownership • Area to record actions and reviews • Review of compliance measuring to: - • Ensure usefulness of data • Ensure accurate use of measuring tool
Objectives & Method of PVC Audit Objectives • Identify the time and date of insertion • Measure the duration that PVC was in place • Document the rationale and reasons for insertion • Identify the reasons for accessing the PVC • Check dressings were intact and met agreed standards • Establish if PVC removed when there was extravasation or inflammation Method • Pilot undertaken Feb 2010 • Audit undertaken May 2010 • 75 completed data collection forms returned
Results Insertion Site 49% 29% 8% 5% 3% 4% 1% PVC Inserted 49% 21% 15% 8% 5% 1%
Results Reason for Access 97% of inserted PVC were accessed 37% 38% 34% 29% 21% 16% 8% < 72 hrs Length of Time Inserted No Response > 72 hrs
Results PVC Dressings 81% Intact 41% IV 3000 48% Tegaderm 1% Pink Elastoplast Tape Resiting of PVC • Phlebitis scoring tool used with the questionnaire • 11% (8) resited • 3 cases of extravasation • 4 cases of dislodged PVC • 1 case removed by patient
Action Plan • Results shared locally at ward and with wider NHS Grampian • Presented at multidisciplinary audit meeting to facilitate discussion and gain agreement on our local plan for the Paediatric PVC Care bundles • Will be using PDSA approach and gathering local ward data but plan to repeat hospital wide audit next year • Share results with wider SPSP Paediatric community at LS7
Next Steps • PVC Bundle • Safety Briefing across Child Health • Debriefing element of perioperative work • Reliable system for inputting data and reporting