Download
1 / 32
320 likes | 489 Views
The Clinical Perspective. A Model Integrated, Guideline-Driven Process Management System . Jason B. Martin, M.D. Vanderbilt Medical Center Nashville, Tennessee, USA. Outline. Who we are The clinical paradigm Electronic support in the ICU Architecture of the tool Implementation

E N D
The Clinical Perspective A Model Integrated, Guideline-Driven Process Management System Jason B. Martin, M.D. Vanderbilt Medical Center Nashville, Tennessee, USA
Outline • Who we are • The clinical paradigm • Electronic support in the ICU • Architecture of the tool • Implementation • Future Directions
The Research Team • Multi-disciplinary collaboration • “A solution in search of a problem” • Objectives • Establish an evidence-based protocol approach • Model the protocol • Create, iterate, and deploy • Measure the benefits and changed practices (we hope)
In Search of a Clinical Paradigm “Do something that matters.” “Study sepsis.” Arthur Wheeler, M.D.
What is sepsis? • Infection : a micro-organism occupies a normally sterile site • Systemic inflammatory response syndrome (SIRS): • temperature > 38 or < 36 • heart rate > 90 • respiratory rate > 20 • WBC count > 12,000 or < 4,000 • Sepsis : the systemic inflammatory response syndrome secondary to a known (or suspected) infection • 3 = 1 + 2
Trauma Burns Infection Sepsis SIRS Pancreatitis Other
Epidemiology • Common • Deadly • Expensive • Treatable • 1-3 cases per 1000 per year • 750,000 cases in the US in 2001 • No age, social, geographic, • or racial boundaries
Epidemiology • Common • Deadly • Expensive • Treatable • 200,000 + US deaths in 2001 • 25-35% mortality
Epidemiology • Common • Deadly • Expensive • Treatable • $17B US • 40% of all ICU costs • 3-5 weeks of hospitalization
Epidemiology • Common • Deadly • Expensive • Treatable • Validated treatment protocols • established
Current Treatment • Surviving Sepsis Campaign • Reviewed, graded evidence; formulated guidelines • Suggests use of treatment protocols and bundles • Multiple interventions • Time-sensitive • Frequent follow-up and re-assessment
The ICU Environment • Information-intensive, stressful environment • Multiple patients • Revolving practitioners • Large volume of data • Temporally discontinuous • Ideal environment for a technology intervention
Hypothesis • Implementation of an electronic process management tool will result in increased adherence to evidence-based practices, improvement in objective quality indicators, and better clinical outcomes for septic patients.
Objectives • Develop a comprehensive clinical protocol for the management of septic patients • Design and deploy the process management tool • Study the impact on physician practices, cost, and patient outcomes
Technical Barriers • Operational protocols, healthcare policies, and treatment guidelines are rarely phrased in a mathematically sound manner • Medical protocols are not “law” • Customizable? • Processes, triggers need to be flexible
Clinical Barriers • Disproportionate impact of anecdotal experience • Failure to appreciate the limits of human decision-making capacity • Exclusion of practitioners from the development process • Tendency to focus on unlikely, but possible, clinical scenarios
Clinical Barriers • Imposing undue burdens on the end-user • Concern about accuracy of protocol elements • Pride among practitioners defending their autonomy
Knowledge-based Systems in the ICU • Commonly available “workflow systems” • Results systems • EMRs • POE • Support systems • Reminders • Pathways • Decision-support • Process management
Decision Support vs. Process Management • Decision Support • Answers to specific questions at independent points • Process Management • Comprehensive guide; has the ability to recalculate if you deviate DS
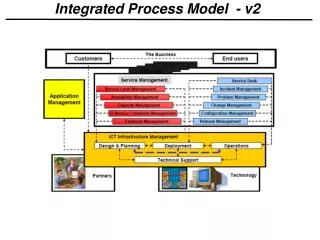
Process Management at Vanderbilt • Vanderbilt is pioneering process management applications in critical care environments • The dashboard approach graphically displays the status of various tasks in a protocol • Has been applied to VAP in ICUs • Preliminarily showing clinical benefits
Our Sepsis Process Management Tool • Integrated with the critical care dashboards • Identifies patients who might have sepsis • Prompts evaluation by clinical teams • If septic, provides real-time management recommendations
Model-based Computing: The Key Enabler • An approach developed at ISIS • Focuses on formal representation, composition, and manipulation of integrated models of information processes, safety / security policies • Provides tools for automated system generation directly from the models
Early Iterations *A Blueprint for a Sepsis Protocol, Shapiro et. al., ACAD EMERG MED d April 2005, Vol. 12, No. 4
Early Iterations • Advantages • Followed formalization efforts available in the literature • Relatively simple • Disadvantages • Did not scale well • Did not properly represent temporal relationships between tasks • Did not accurately reflect physician thinking
Later Iterations • Divide the protocol into discrete processes • Processes organized in a hierarchical manner and are activated with specific conditions • Processes are concurrent, asynchronous, and can interact via events • Processes “isten” for events that satisfy entry conditions • This scheme solved earlier problems and was more intuitive for physicians
Later Iterations *A Blueprint for a Sepsis Protocol, Shapiro et. al., ACAD EMERG MED d April 2005, Vol. 12, No. 4
Summary • Evidence-based clinical protocols are becoming the ‘gold standard’ of clinical best practice • To be effective, protocols must be deployed as a formal, customized/individualized clinical care plan • Model-driven generation is a very effective strategy for converting protocols into plans • Integration into team-based clinical practice is needed to test clinical effectiveness
Acknowledgements • Clinical Contributors • Liza Weavind • David Maron • Gordon Bernard • Art Wheeler • Todd Rice • Human Factors • Anne Miller • Center for Clinical Improvement • Shea Polancich • Shirley Primeau • Byron Lee • Health Tech Lab • Peter Miller • ISIS • Janos Sztipanovits • AkosLedeczi • Janos Mathe • AndrasNadas • Informatics • Dan Albert • Norm Deane • John Paulett • Rachel Hayes