Download
1 / 29
290 likes | 531 Views
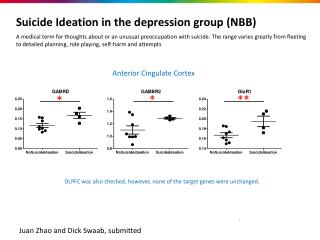
NBB. (Neurological-Based Behaviour). By: Suzanne Dondo Erin Ellison Ryan Pariseau. Paula Cook – Chapter 3. Definition.

E N D
NBB (Neurological-Based Behaviour) By: Suzanne Dondo Erin Ellison Ryan Pariseau Paula Cook – Chapter 3
Definition • Neurological Based Behaviour (NBB) is a term used to describe a number of different DIAGNOSIS, in which an individual cannot RELIABLY be held accountable for their actions (e.g. what they say and do). • Approximately 10% of all students are estimated to be affected by NBB. (Cook, 2008)
Types of NBB • Brain injuries • signs and symptoms vary depending on the location of the damage • ADHD • ODD • Bipolar Disorders • Anxiety Disorders • Learning Disabilities • Alcohol Related Neurological Disorders • Sensory Integration Dysfunction (SID) • Autism Spectrum Disorders (ASD) • Rage Note: Medications can be very effective for certain individuals but should be used in conjunction with other strategies.
Sensory Integration Dysfunction (SID) • A condition that varies in severity and impacts one or more of the following body senses: • Auditory • Visual • Olfactory • Gustatory • Tactile • Vestibular (balance and movement) • Proprioreceptive sense (sense of position) • Each can be either HYPERSENSITIVE, HYPOSENSITIVE or BOTH (Cook 2008)
Signs • Hyperactivity (excess energy) • Inattentive • Fidgety • Learning difficulties • Coordination problems • Behaviour difficulties • Inability to unwind and calm themselves • Language difficulties • Impulsive or lack of self-control • Disorganized (Cook 2008)
Things we can do • MODIFY the environment (first) • Make direct observations of a student (with SID) in several different environments, to identify sensory needs • Increase student awareness of sensory influences and build in coping strategies • Create sensory friendly options for students (Cook 2008)
Critical Point • How do you teach appropriate verses inappropriate sensory coping strategies?
Autism Spectrum Disorders • Is a condition in which individuals show signs of the following (degree differs amongst individuals): • Problems interacting socially • Communicating • Understanding intentions • Building and maintaining relationships • Problems understanding concepts and language (literal thinkers) • Self involved • Lack of eye contact • Repetitive behaviours (stimming, perseverating, repeating)
Things we can do • Modify the environment to meet sensory needs (helps individuals deal with overstimulation and under stimulation) • Social Stories • Using board maker picture symbols • Comic book version • Video modeling • Switching between high interest and low interest activities (can be used to develop strengths and work on areas that require strengthening) • Use visual teaching strategies • Use of positive reinforcement
Critical Point • Teaching acceptance verses tolerance
Rage • Rage is an unexpected explosion of temper that can turn violent (Parker, 2005) • It is a process that should be understood as a traumatic neurological event that cannot be controlled by the student. • The limbic system reacts before the language and reasoning part of the brain becomes fully engaged. This is important to understand so that we realize that talking things out often makes things worse.
Critical Point How do we differentiate between Neurological Based Behaviour and willful misbehaviour?
Differences between temper tantrums and rage Temper Rage Rage releases built up tension or frustration. Once rage begins, there is little a person can do to stop it. As the rage is running its course, adults may be able to help control or soften the behaviour to some degree. Rage can last from a few minutes to a few hours. • Tantrums are goal oriented. The temper has a purpose of getting something or getting someone to do something. • Tantrums can turn to rage.
Rage cycleRage runs through a five stage cycle: pre-rage, triggering, escalation, rage, post rage. Phase 1: Pre-rage: This is the time before the rage has been triggered.
Phase 2: • Triggering stage: An event or situation occurs to trigger an escalation of behaviour causing a flight, fright, freeze response. • The triggering situations could be the following: • Work transitions, • Sensory overload, • Being told no, • Fatigue, • Frustration, • Confusion, • Hunger.
Phase 3: Escalation • The trigger has created chemical changes in the brain to cause the person to go into a fight/flight/freeze (escalation) reaction. • Evidence of mild escalation: • Begin to get angry; • Body language is tense; • Appears to be startled in their physical or verbal responses; • Start speaking louder or yelling; • Talk quickly; • Call inappropriate names or use inappropriate language. • Evidence of rapid escalation: • Demonstrate mood changes. • Body language is tense; • Become flushed, clammy or perspire • Visibly shake • Make threatening gestures such as shaking a fist, throwing furniture/objects or use aggressive language such as I hate you, I will kill you; • Try to leave area or run away.
Phase 4: Rage is the outcome of neurological and physical changes. • To document the rage episodes, note the following: • The event leading to the rage episode; • The length of rage; • The intensity of the behaviour cycle. • The physical actions: Use descriptive language such as “while Suzanne was playing soccer with her classmates; she picked up the ball, glared at another child in the class with an angry expression on her face for a few seconds and threw the ball at this child”. • The verbal threats or comments • The interventions or strategies that worked to de-escalate or to sooth the child. • Over a period of time, analyze the number of rages per day, per week, per month, the triggers, the intensity of the rages and the successful interventions.
Dos and Don’ts of intervening rage Dos • Allow the person to go through the cycle. • Keep everyone else safe by clearing them out of the room or by signaling them to ignore behaviour. • Use non confrontational body language. Stand on an angle, off center with legs one meter apart, your hands by your body, blocking any eye contact between others in the room and the person escalating. • Use a calm, quiet, non emotional voice and supportive, empathetic language • Calmly, quietly provide short, concise language to change behaviour. • Go to quiet room (A predetermined safe place). • Breath in through your nose and out through your mouth. • Hands on belly. • Praise as soon as the person starts following a direction. • Redirect or divert attention. • Sometimes, walking away will help calm them down. • If necessary, call another adult who has a stronger rapport with the student or has more experience with de-escalating rages. • Document rage: note the length of the rage, the triggers, etc.. Don’t • Take it personally; • Physically restrain unless people are unsafe. • Yell, scream or to talk the person out of the rage, or use sarcasm. • Address inappropriate language, threats, gestures at this time; • Cross your arms at your chest or put your hands on your hips.
Phase 5: Post – rage: • Cook cautions us that a rage cycle takes a lot of energy from the person experiencing these neurological and physical changes. After a rage, the person may or may not remember the event. • Behaviours after a rage: • Disoriented or confused; • tired; • Physically exhausted; • Passive; • Calm; • In pain, may have a headache or aches/pains in their body; • apologetic, remorseful or embarrassed; (maybe) • Ready to continue their day; • Sleepy. Cook suggests to let the person sleep for awhile before debriefing.
Post –rage interventions Interventions following the rage cycle. • Remind the person that they are safe. • Allow the person time to relax, sleep, or be alone. • Do not talk about consequences. Cook feels that it is the same as disciplining someone for having a heart attack or a diabetic shock; • Allow the person to put the rage behind them. When the child is ready, use this time as a teaching opportunity: • May discuss about “how to make things smaller” or “fixing things up”. • Help the child put the event into language. • Plan with the child things to do next time a rage occurs: • Finding a safe, sensory soothing place to go, • Use words to get what they want, • Timing themselves out.
Discussion Well it (inclusion) hasn’t worked. Classrooms are disrupted, teachers are stressed and students who need help don’t get it. The BCTS won’t say anything, and neither will the government, for fear of being accused of being callous and indifferent to students with special needs. As far as I am concerned, the school system has given the mainstream model a fair chance. It doesn’t work. Time to try the alternative.” (Ian Cameron, Victoria Times Colonist, September 23, 2005) • How can the classrooms be better supported so that inclusion is not seen as a burden to the schools? • Does the inclusion model means that every child regardless of their needs and behaviours be placed in a mainstreamed class? • What protocol or criteria should we follow in deciding the best learning environment for the child?
Discussion The message of zero tolerance is politically appealing, giving parents and communities the perception that schools are being tough on behaviours. • How does the zero tolerance policy drive the administration’s disciplinary decisions when dealing with students with NBB who exhibit rage issues? • How does the zero tolerance policy affect the perceptions of our paraprofessionals/teachers assistance/teachers? • How can we change these perceptions?
Training Teachers / Educational Assistants • Build Capacity through education • Staff meetings • Book studies • Explore beliefs • Collaboration & Support
Dr. Jennifer Katz (Universal Design), March 2010 Building Classroom Climate/Community Multiple Intelligence Training Peers are responsible for each other
Training Peers: • Explicit instruction regarding different abilities • Literature • Presentations • Websites • Strategies (Pivotal Response Training – PRT) • Circles of Friends
Supporting Friendships • Encouraging a friend to play with the child at home. • Help student join clubs, with support as needed. • Teaching the child to observe other children’s positive behaviour and imitate them. • Encouraging cooperative games. • Modeling how to relate to the child and educating other students in the class to do the same.
Encouraging prospective friendships. • Providing enjoyment at break times. • Doing projects and activities that illustrate the qualities of a good friend. • Helping the student to understand emotions through direct teaching of how to read people’s faces and body language and respond to cues that indicate different emotions.
People First • Teachers/EAs – Look at the whole • Peers - The Golden Rule
Bibliography • Cooke, P. (2008) Rage: A layperson’s guide to what to do when someone begins to rage. To order pamphlet e-mail: pcooke59@shaw.ca • Cooke, P. (2008) The special challenges of neurological-based behaviour. Charles, C. (ed) Building classroom discipline. (pges. 34-53) Boston, MA: Pearson Education Inc.