Download
1 / 43
900 likes | 3.66k Views
Spinal Cord lesions. Prepared by : Saad Al-Qahtani. Presented by : Bandar Al-Qahtani. Supervised by : Dr.Esam Al-Jamal. Anatomy . Spinal cord lies within protective covering of vertebral column. Begins just below foramen magnum of the skull. Ends opposite 2 nd lumbar vertebra.

E N D
Spinal Cord lesions Prepared by : Saad Al-Qahtani. Presented by : Bandar Al-Qahtani. Supervised by : Dr.Esam Al-Jamal.
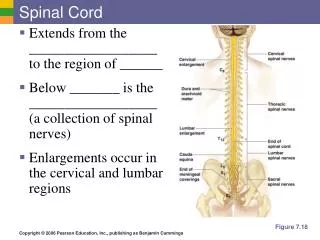
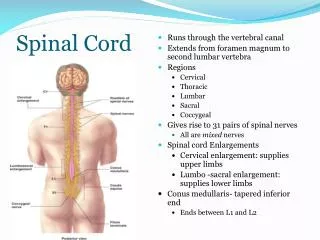
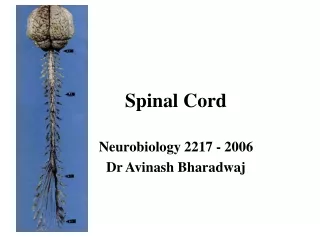
Anatomy • Spinal cord lies within protective covering of vertebral column. • Begins just below foramen magnum of the skull. • Ends opposite 2nd lumbar vertebra. • Below L2 continue as a leash of nerve roots known as cauda equina. • Prolongation of the pia matter forms filum terminale.
Spinal cord structure • The spinal cord consists of central core of grey matter containing nerve cell bodies, and outer layer of white matter of nerve fibers. • Within the grey matter, the dorsal horn contains sensory neurons, the ventral horn contains motor neurons and the lateral horn contains preganglionic sympathetic neurons. • Within the white matter run ascending and descending nerve fiber tracts, which link the spinal cord to the brain.
Spinal cord structure • The principle ascending tracts are the spinothalamic tracts, spinocerebellar tracts and dorsal columns. The coticospinal tracts is an important descending tract. • The spinal cord receives information from, and controls the trunk and limbs. • This is achieved through 31 pairs of spinal nerves which join the cord at intervals along its length and contain afferent and efferent nerve fibers connecting with the structures at the periphery.
Causes of spinal cord lesions • congenital; spinal stenosis. • Infection; TB ,abscess. • Trauma; vertebral body fracture or facet joint dislocation. • Inflammatory; Rheumatoid arthritis. • Disc and vertebral lesion. • Vascular; epidural and subdural hemorrhage. • Tumors.
Spinal stenosis • 75% of cases of spinal stenosis occur in the low back ( lumbar spine). • Causes : - congenital. - degenerative. - trauma.
Congenital spinal stenosis • The patient is born with a narrow spinal canal due to abnormally formed parts of the spine. • This condition is most common in patients with a short stature, such as achondroplastic dwarves.
Other causes of spinal stenosis • aging process(most common cause ). • herniated discs. (fig) • bone and joint enlargement. • spondylolisthesis. • bone spurs.
Rx Spinal Stenosis • Initial Rx in most cases is conservative. • Rest. • Weight loss. • Epidural steroid injections. • Analgesia. • Anti-inflammatory agents. • Muscle relaxant -if needed- • Physiotherapy.
Rx spinal stenosis • Spine surgery: used when conservative treatment failed. -laminectomy (removing bone behind the spinal cord). -foramenotomy (removing bone around the spinal nerve). -discectomy (removing the spinal disc to relieve pressure). Complications: Dural tears. Infections. Instability of the spine.
Infection • Epidural abscess • Usually bacterial ( staphylococcus is common). • Spread through: • hematogenous route. • Adjacent focus. • Direct inoculation.
Risk factor for epidural abscess • immunodeficiency • AIDS. • Alcoholism. • Chronic renal failure. • Diabetes mellitus. • Intravenous drug abuse. • Malignancy. • Spinal procedure or surgery. • Spinal trauma.
Infection • Infection of spine • Uncommon • Either vertebral osteomyelitis Or less commonly intraspinal infection. • Causative organism : (staph, Strep, E.coli, TB) • Occasionally due to unusual organisms like: Salmonella or brucella.
Rx spinal infections • The goals of treatment are to relieve spinal cord compression and cure the infection. -drain abscess. -antibiotics or antimicrobial. -corticosteroid. -may need urgent surgical decompression by laminectomy.
Tumors • Tumors are classified into 3 types according to their site: -extradural ( between the meninges and spine bones) -intradural extramedullary (within meninges) -intramedullary ( inside the cord)
Spinal tumors • Most spinal tumors are extradural – about 85% • They may be primary tumors originating in the spine, or secondary tumors that are the result of the spread of cancer from other locations primarily the lung, breast, prostate, kidney, or thyroid gland. • Any type of tumor may occur in the spine, including lymphoma, leukemic tumors, myeloma, and others. A small percentage of spinal tumors occur within the nerves of the spinal cord itself, most often consisting of ependymomas and other gliomas.
Symptoms of spinal tumors • Pain (in 90% of patients), numbness or sensory changes, motor problems and loss of muscle control. • Pain can feel as if it is coming from various parts of the body. • Numbness or sensory changes can include decreased skin sensitivity to temperature and progressive numbness or a loss of sensation, particularly in the legs. • Motor problems and loss of muscle control can include muscle weakness, spasticity (in which the muscles stay stiffly contracted), and impaired bladder and/or bowel control.
Spinal tumors • 17% have Multiple level involvement. • Metastatic lesion mostly found in Thoracic spine. • Myelopathy develops over days to weeks. • Acute SCC does occur if tumor enlarges very rapidly due to hemorrhage or if a vertebral body suddenly collapses.
Extradural tumors • The most common spinal tumor – 85% • mostly metastatic. • Arise from osseous element of spinal column. • Grow rapidly. • Primary ; Lung, Breast, prostate and kidney. • Compress the spinal cord by Growing in epidural space Causing collapse of vertebrae, distortion and narrowing. e.g. lymphoma, hemangioma and neuroblastoma.
Intradural extramedullary tumors • Inside the dura but outside the spinal cord. • e.g. Meningioma, Neurinoma. • Arise from the dural sheath around the cord or showann cell sheath around the spinal root. • Multiple tumors in Pt. with neurofibromatosis. • Can grow extradurally into retropleural or retroperitoneal through intervertebral foramen.
Intradural intramedullary tumors • Inside the spinal cord • Examples: Glioma, ependymoma, astrocytoma • Arise from glial elements of spinal cord or trapped ectodermal elements. • More common in children. • Astrocytoma of spinal cord is the most common intramedullary tumor of childhood. • Ependymoma of spinal cord is the most common intramedullary tumor of adulthood. • Arise from ependyma of central canal. • Well demarcated.
Investigations • Plain X-rays. • Myelography “contrast material is injected into the thecal sac fluid surrounding the spinal cord and nerve root within the spinal canal” • CT. • MRI ( study of choice ).
Rx spinal tumors The goal of treatment is to reduce or prevent nerve damage from compression of the spinal cord, relieve pain and maintain the function. - Surgical excisionis the treatment for extramedullary tumors. - Radiation therapyfor intramedullary tumors. The traditional treatment of intramedullary gliomas has been biopsy followed by radiation therapy. Radiotherapy is clearly of value in metastatic lesions. - Chemotherapycan be considered in patients with progression of disease after radiation therapy.
Spinal cord compression (SCC) • The act of exerting an abnormal amount of pressure on the spinal cord. • Causes and risk factors : - Traumatic injury. - Spinal cord tumors. - Spinal stenosis. - Ruptured disks. - Abscesses. - Arteriovenous malformations. - Degenerative diseases, such as arthritis.
Clinical presentation Symptoms vary depending on the cause of the compression, its location, severity, extent and rate of development but can include: - Back pain at the spinal site of compression. - Pain or burning in other parts of the body. - Difficulty breathing. - Weakness in the arms, legs, or both. - Numbness or tingling in the neck, shoulder, arms, hands, or legs. - Loss of coordination or difficulty walking. - Loss of fine motor skills. - Loss of sexual function. - Loss of bladder or bowel control. - Paralysis.
Clinical presentation - Cervical spine disease produce Quadriplegia. - Thoracic spine disease produce paraplegia. - TENDON REFLEXES • Increase; below level of compression • Absent; at the level of compression • Normal; above the level of compression - Sphincter disturbances are late feature of cervical and thoracic cord compression.
Clinical presentation • Cauda equina syndrome; is a serious condition caused by compression of the nerves in the lower portion of the spinal canal . is considered a surgical emergency because if left untreated it can lead to permanent loss of bowel and bladder control and paralysis of the legs.
Investigation • X ray. • CT scan. • MRI. • Myelogram. • Biopsy. • Bone scan. • Blood and spinal fluid studies.
Rx spinal cord compression • Acute cord compression is a 'surgical' emergency. • In those with malignant disease radiotherapy may be treatment of choice. • In general, tumor, infection and disc disease produces anterior compression. • Surgical decompression should be achieved through an anterior approach.
Spinal trauma • Spinal cord trauma is damage to the spinal cord. It may result from direct injury to the cord itself or indirectly from damage to surrounding bones, tissues, or blood vessels. • Symptoms: Symptoms vary depending on the location of the injury. Spinal cord injury causes weakness and sensory loss at and below the point of the injury. we can divide spinal trauma into 3 levels according to its location in the spinal cord ( cervical - thoracic – Lumbosacral ).
Cervical injuries - When spinal cord injuries occur near the neck, symptoms can affect both the arms and the legs: • Breathing difficulties (from paralysis of the breathing muscles). • Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). • Numbness. • Sensory changes. • Spasticity (increased muscle tone). • Pain. • Weakness, paralysis.
Thoracic injuries - When spinal injuries occur at chest level, symptoms can affect the legs: • Breathing difficulties (from paralysis of the breathing muscles) • Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). • Numbness. • Sensory changes. • Spasticity (increased muscle tone). • Pain. • Weakness, paralysis. • Injuries to the cervical or high-thoracic spinal cord may also result in blood pressure problems, abnormal sweating, and trouble maintaining normal body temperature.
Lumbosacral injuries - When spinal injuries occur at the lower-back level, varying degrees of symptoms can affect the legs: • Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). • Numbness. • Pain. • Sensory changes. • Spasticity (increased muscle tone). • Weakness and paralysis.
Investigations • A CT scan or MRI of the spine may show the location and extent of the damage and reveal problems such as blood clots (hematomas). • Myelogram (an x-ray of the spine after injection of dye) may be necessary in rare cases. • Somatosensory evoked potential (SSEP) testing or magnetic stimulation may show if nerve signals can pass through the spinal cord. • Spine x-rays may show fracture or damage to the bones of the spine.
Rx Spinal trauma • ABC • Spine Immobilization to prevent further injury to the spinal cord. • In cervical injuries higher than C5, intubation and respiratory support are usually needed. • Corticosteroids, rest, analgesics and muscle relaxant. • Surgery (decompression laminectomy ). • Extensive physical therapy and other rehabilitation interventions are often required after the acute injury has healed.
Disc prolapse Rupture of the disc or prolapse as it is usually called, can press on the spinal cord and its nerve roots leading to pain, numbness and weakness and may also affect the control of bowel and urinary bladder. Dx: X-ray, CT scan or MRI.
Rx Disc Prolapse • Initial Rx in most cases is conservative. • Rest. • Analgesia. • Anti-inflammatory agents. • Muscle relaxant -if needed-. • Physiotherapy.
Rx Disc Prolapse • laminectomy, involves excision of a portion of the lamina and removal of the protruding disk. • spinal fusion, may be necessary to overcome segmental instability. • Laminectomy and spinal fusion are sometimes performed concurrently to stabilize the spine. • Microdiskectomy, can also be used to remove fragments of nucleus pulposus. • Chemonucleolysis:Injection of the enzyme chymopapain into the herniated disk produces a loss of water and proteoglycans from the disk, thereby reducing both the disk’s size and the pressure in the nerve root.
Spondylolisthesis • Spondylolisthesis is a condition in which the there is a defect in a portion of the spine, causing vertebra to slip to one side of the body.
Rx Spondylolisthesis • Non-surgical treatment may include one or a combination of: - NSAID’s (e.g. ibuprofen, COX-2 inhibitors) - Oral steroids - Physical therapy - Manual manipulation (e.g. chiropractic manipulation). • Spinal fusion surgery.