Download
1 / 22
260 likes | 670 Views
HEMORRHAGE RESUSCITATION AND MASSIVE TRANSFUSION PROTOCOLS. CAPT William C. Brunner, MC, USN Senior Medical Officer, BSRF-2013 Assistant Professor, Department of Surgery. Disclosures.

E N D
HEMORRHAGE RESUSCITATIONANDMASSIVE TRANSFUSION PROTOCOLS CAPT William C. Brunner, MC, USN Senior Medical Officer, BSRF-2013 Assistant Professor, Department of Surgery
Disclosures The speaker has no relevant financial relationships with commercial interests that pertain to the content of this presentation
Objectives • Review History of Trauma Resuscitation • Discuss Coagulopathies in Trauma • Discuss Integrated Damage Control • Review Blood Component Preparations • Discuss Individual Component Transfusion Guidelines • Discuss Massive Transfusion Protocols • Discuss Future Research Areas
History of Trauma Resuscitation • World War I • Little or no systematic resuscitation after injury • Blood banking developed • World War II • Widespread use of blood and albumin • Long, slow evacuation • Significant organ failure – renal, pulmonary • Late deaths from sepsis
History of Trauma Resuscitation • Korean War • Forward Surgical Care • Rapid Care • Evacuation to Definitive Treatment • Blood and albumin as in WWII • Vietnam War • Rapid evacuation • Large-volume resuscitation with blood/crystalloid • Da Nang Lung (ALI/ARDS)
History of Trauma Resuscitation • Civilian Experience • Trauma Registries and Research • Empiric high-volume crystalloid resuscitation • Iatrogenic Coagulopathy after Trauma recognized • Directed Component Therapy • Requires Laboratory evidence • Empiric therapy limited • Massive Transfusion Protocols
History of Trauma Resuscitation • Military Experience – Iraq and Afghanistan • Limited Component availability • Recognition of crystalloid inflammatory response • Whole blood transfusion • Walking Blood Bank • Simple technology • Screened donor population readily available
Acute Traumatic Coagulopathy • Recognized in patients with significant tissue injury and hypotension • Distinct from iatrogenic coagulopathy after trauma • Dilutional coagulopathy • Present prior to resuscitation in rapidly evacuated severe trauma • Mortality rate increased 4x • Modulated through protein C activation
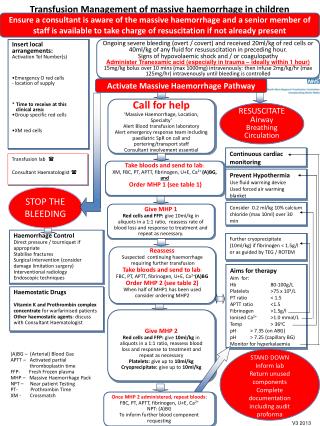
Integrated Response • Damage Control Surgery • Rapid, limited, forward surgical care • Control bleeding • Control spillage • Control contamination • Restore perfusion • Avoid unnecessary interventions • Allow for resuscitation • Rapid evacuation • Hemostatic Resuscitation • Limited volume • Permissive hypotension • Balanced transfusion • High FFP:PRBC ratio • Colloid vs. crystalloid • Attenuate ATC • Expand resource availability • Walking blood bank • Freeze-dried plasma
Component Therapy • Advantages • Wider use of limited resources • 1 donated unit – multiple products • Longer storage life • Lower costs in elective use • More predictable availability • Disadvantages • Multiple donor antigen exposure • Less efficacy in high volumes, Lab costs
Component Transfusion Guidelines • Fresh Frozen Plasma • Prothrombin Time (PT) > 17 sec • Clotting Factor Deficiency (<25% of normal) • Massive Transfusion (1 unit/5units RBCs) or clinically bleeding • Severe Traumatic Brain Injury • Cryoprecipitate • Fibrinogen < 100mg/dL • Hemophilia A, von Willebrand disease • Severe Traumatic Brain Injury
Component Transfusion Guidelines • Platelets • Platelet count < 10,000/uL • Platelet count 10,000 to 20,000 with bleeding • Platelet count < 50,000 after severe trauma • Bleeding Time > 15 mins • Platelet concentrates (5.5 x 1010 in 50ml) • Platelet apheresis (3 x 1011 in 300ml)
Component Transfusion Guidelines • Packed Red Blood Cells (PRBCs) • Hemoglobin < 7g/dL • Acute blood volume loss > 15% • > 20% decrease in BP, or BP <100mm Hg due to blood loss • Hemoglobin < 10g/dL with significant cardiac disease or symptoms (chest pain, dyspnea, fatigue, orthostatic hypotension) • Hemoglobin < 11g/dL in patient at risk for MOF
Massive Transfusion • Defined as > 10 units PRBCs within 24 hrs • 25-30% of trauma patients requiring massive transfusion will present with Acute Traumatic Coagulopathy (ATC) • Penetrating mechanism • Positive FAST • Arrival SBP < 90mm Hg, HR > 120 bpm • Unstable pelvic fracture • pH < 7.25, base deficit
Massive Transfusion Protocol • Advantages • More closely replicate whole blood physiology with components • Retain shelf-life advantage of components • 25-30% reduction in PRBCs used • Predictable workload • Disadvantages • Processing time limitations • Limited applicability
Massive Transfusion Protocol Data from O’Keeffe T, Refaai M, Tchorz K, et al: A massive transfusion protocol to decrease blood component use and costs, Arch Surg 143:686-691, 2008.
Massive Transfusion Protocol • Typically start with 2-6 units Type O blood • Initial “emergency-release” • Subsequent units type-specific, cross-matched • FFP processing time • ER prestaging thawed plasma, shelf-life 4-5 days • Protocols can enhance effective use of staffing and resources
Special Situations • Autotransfusion • Limited applicability due to capture, possible contamination • Blood salvage • Intraoperative or postoperative • Labor intensive, expensive, limited utility • Autologous donation, Hemodilution not applicable to trauma setting
Areas for Future Study • Determine optimal therapeutic ratio of PRBC:FFP • PROPPR Study - 1:1:1 vs. 1:1:2 PRBC/PLT/FFP • Further delineate ATC physiology and identify clinically useful modulators • Delineate impact of high-ratio therapy on sub-MT trauma population • Blood component substitutes • Crystalloid alternatives
References • McIntyre RC Jr., Moore FA; Blood Transfusion Therapy, Chapter 212, Current Surgical Therapy, 10th Edition, Philadelphia, PA, 2011. • Adams CA Jr., Stephen A, Cioffi WG; Surgical Critical Care, Chapter 23, Sabiston Textbook of Surgery, 19th Edition, Philadelphia, PA 2012. • Chovanes J, Cannon JW, Nunez TC; The Evolution of Damage Control Surgery, SurgClin N Am 92 (2012) 859-875.
References • Cohen MJ. Towards Hemostatic Resuscitation: The Changing Understanding of Acute Traumatic Biology, Massive Bleeding, and Damage-Control Resuscitation. SurgClin N Am 92 (2012) 877-891. • Committee on Trauma, American College of Surgeons. ATLS: Advanced Trauma Life Support Student Course Manual, 9th Edition. Chcago: American College of Surgeons; 2012.