Download

1 / 38
390 likes | 627 Views
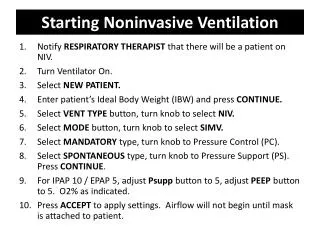
The Latest Developments in Noninvasive Mechanical Ventilation. Nicholas Hill MD Tufts Medical Center Boston, MA USA. Disclosures. Research Grants Respironics, Inc Breathe Technologies, Inc. Outline. ICU Applications of NIV Main indications COPD, Pulm Edema ALI/ARDS

E N D
The Latest Developments in Noninvasive Mechanical Ventilation Nicholas Hill MD Tufts Medical Center Boston, MA USA
Disclosures • Research Grants • Respironics, Inc • Breathe Technologies, Inc
Outline • ICU Applications of NIV • Main indications • COPD, Pulm Edema • ALI/ARDS • Extubation Failure, Trauma • Epidemiology of use • Practical Application • Masks, Ventilators
Why Noninvasive Ventilation? • Avoids trauma of intubation • Reduces respiratory infections • More comfortable, less sedation • Less costly • Respiratory System Protective Strategy • Must be used selectively
Main Indications for Acute Noninvasive Ventilation (NIV) Strong (Level A) Acute hypercapnic RF (COPD) Cardiogenic pulmonary edema ARF in immunocompromised
NIV for COPD associated with: • Difficult weaning (to facilitate extubation) • Pneumonia • Extubation failure • Do-not-intubate status • Post-operative Respiratory Failure
NIV for Acute Pulmonary Edema: Physiologic Rationale • CPAP: • Increased FRC • Re-expands flooded alveoli • Improved oxygenation • Increased compliance • Afterload reduction - cardiac function • Pressure Support: • Further reduction in work
Meta-analysis: CPAP vs NIV for ACPE “Evidence …is now robust…and use as a first line intervention is becoming mandatory.” Winck et al, Crit Care 2006 10:R69
Out-of-Hospital CPAP Vs Usual Care in Acute Respiratory Failure: A RCT Thompson et al,Ann Emerg Med. 2008;52:232-241 CPAP Control (10 cm H2O) n 35 34 SaO2 82% 75% RR/min 38 38 CHF/COPD/Asthma 99% 100% Intubation 7(20%) 17(50%)* Hosp Mortal (%) 4(14%) 12(35%)* *P<0.05
Indications for Acute NIV Weaker (Level B) Asthma Extubation failure(COPD) Hypoxemic Respiratory Failure Postoperative Respiratory Failure Do-not-intubate pts (COPD and CHF)
RCT of NPPV for Asthma Exacerbations • NPPV Sham • n 17 16 • FEV1 (%) 37.3 33.8 • 50% FEV1 (1h) 80% 20%* % FEV1 (1h) 53.5 28.5* Hospitalized 3 (17.6%) 10 (63.5%)* Soroksky et al, Chest 2003; 123:1018.
Use of NIV as Bronchodilator ∆ FEV1 % 8/6 cm H2O 6/4 cm H2O O2 by FM 44 asthmatics, FEV1 33% P 80-90, RR 20 3 Groups, “High”, “Low” and O2 ctls for 1hr Hydrocort BUT NO BDs! Soma T et al, Intern Med ‘08
NIV for Asthma Used for pts with “status asthmaticus” – severe and refractory to treatment May combine with continuous neb and heliox (anecdotal evidence) Monitor very closely ? Role early for bronchodilator effect and to reduce dyspnea more rapidly?
NIV for Hypoxemic Resp Failure? 72 yo M with 3-4 days dyspnea, fever, chills, dry cough. No chest pain, takes beta blocker for HBP. In the ICU, moderately dyspneic, RR 30. Not using access muscles. BP 146/80, P 92, O2 Sat 98% on 40% Facemask. No JVD, lungs - bilat crackles, heart no m, g; no edema. ABG on 40% FM is 7.36/42 PaCO2/100 PaO2. Renal, liver fxn nl. CXR - bilat interstitial infiltrates, new since 3 mos earlier, EKG shows ST with NSSTTs. Diagnosis: Community-acquired pneumonia Does he have ALI/ARDS?
What to do? O2 Alone CPAP NIV Intubate
Poor Outcomes of ALI/ARDS/ Pneumonia treated with NIV Pneumonia associated with poor outcome with NIV – Ambrosino N, Thorax ’95 Severe CAP (RCT) – Better outcomes only in COPD pts with ALI/ARDS – Confalonieri M et al, AJRCCM ‘99 Severe CAP – initial oxygenation better, 66% need for intubation – Jolliet P et al, ICM 2001 ARDS – 38/54 (70%) intubation. P/F 147 success; 112 failure; all septic shock failed – Rana S et al, Crit Care ‘06 The Last Frontier
Acute Hypoxemic Respiratory Failure Italian multicenter study of 354 NIV cases, 30% failures; 50% ARDS or CAP, 10% cardiogenic pulmonary edema Condition Odds Ratio ARDS or Comm Acq Pna 3.75 PaO2:FIO2 146 p 1st hr 2.51 SAPS II 35 1.81 Age > 40 1.72 PaO2/FIO2 < 200 Resp Distress, RR > 30-35 Non-COPD dx Pneumonia (incl immunosuppr) ARDS Trauma Cardiogenic Pulm Edema Antonelli et al, Int Care Med 2001 27:1718
Why is NIV in ALI/ARDS so challenging? • Severe oxygenation defect – more PEEP, more leak, desaturation if mask “falls” off • High minute volumes, tachypnea – harder to meet demands, synchronize • Stiff lungs – Higher insp pressure, more leak, less comfort • Sick patients – sepsis, secretions, MODS, deteriorating
NIV as “First Line” Therapy in ARDS • 147 pts eligible of 479 (332 intubated), had dyspnea, RR > 30 and ≤ 2 new organ failures • 54% avoided intubation – VAP rate 2 vs 20%, mortality 6 vs 53% • Success more likely if SAPS II ≤ 34 and PaO2/FIO2 > 175 p 1st hr of NIV therapy Antonelli et al, CCM, 2006
RCT:Does “Early” Use of NPPV for ALI prevent ARDS/ARF? Incl: 200 < PaO2/FIO2 < 300, FIO2 ≤ 50%, Resp Distress Excl: Age > 70, PaCO2 > 50, GCS <11. SOFA > 2 10 ctrs –stopped early Zhan Q et al, CCM 2012
“Early” Use of NPPV for ALI NPPV (17/6.5) O2 n 21 19 Males 76% 42%* Intub (need/actual) 1/1 7*/4 Organ Failures 3 14* Death 1 5 Stay (ICU/Hosp d) 5.9/17.5 7.8/23 *P < 0.05 Zhan Q et al, CCM 2012
“Early” Use of NPPV for ALI Zhan Q et al, CCM 2012
What would you do now?Do you see a role for “prophylactic” NIV in ALI? O2 Alone? NIV?
Who might get NIV for ALI/ARDS? • Careful selection! • Excellent candidate for NIV – no multiorgan system disease, cooperative, no excessive secretions – SAPS ≤ 34 • Can oxygenate adequately on NIV (FIO2 to 60%); FIO2/PaO2 improves quickly (1st hr) (>150-175) • Skilled center with experienced physicians, respiratory therapists and nurses
Esteban: PaCO2 > 45 MV>48h Resp muscle “fatigue” RR > 25 pH < 7.35 O2sat < 90%, PaO2 < 80 Nava PaCO2>45, MV>72h* >1 failed weaning attempt* excess secretions* upper airway disorder* • NIV for Extubation Failure • 2004 trial - no reduction in reintub- • ations and mortality in NIV group • -Esteban et al, NEJM ’04 • Recent RCT showed resp failure and • 90 d mortality in hypercapnics on NIV • -Ferrer et al, Lancet ‘09 • Don’t delay needed intubation! Selection Criteria in Trials to Prevent Extubation Failure Ferrer: Age > 65, CHF, APACHE score > 12
Non-invasive ventilation reduces intubation in chest-trauma related hypoxemia: A RCT Hernandez et al, Chest 2010; 137:74-80 NPPV Control n 25 25 PaO2/FIO2 108 110 APACHE II 17.5 14.1* Intubation 3(12%) 10(40%)* Exhaustion 2(8%) 6(24%) VAP 2(8%) 3(12%) Hosp LOS (days) 14 21* Hosp Mortal (%) 1(4%) 1(4%) *P<0.05
NIV Epidemiology – How are we doing?Increasing Use of NIV in French and US ICUs % of Pts Carlucci et al, AJRCCM, 2001; Demoule et al, ICM, ’06; Ozsancak et al, Chest ‘08
Use of NIV for COPDMassachusetts and Rhode Island % of Vent starts for COPD exacerbations treated with NIV
Increasing Use of NIV for COPD in US • Healthcare Cost and Utilization Project’s Nationwide Inpatient Sample 1998-2008 • 7,511,267 Admissions for exacerbations • NIV increased 1% to 4.5% of admissions (468% increase) • Invasive Vent dropped 42% from 6% to 3.5% of admissions Chandra D et al, AJRCCM 2012
Increasing Use of NIV for COPD in US (> 7X106 admissions) Chandra D et al, AJRCCM 2012
Diminishing Mortality Overall Chandra D et al, AJRCCM 2012
Forehead Adjuster
RCT: TotalTM vs Full Face Mask 60 pts with ARF on NIV • No difference in • time for application • 8 switched from TFM • to FFM, none FFM • to TFM Ozsancak A et al, Chest 2011
Bilevel Vents for Acute Applications (80% US) NIV modes on Critical Care Vents Leak compensation Adjustable Rise Time Inspiratory Time Limit Silence nuisance alarms Need adjustments if leaks Ferreira, Chest ‘09
NIV Modes on Critical Care Ventilators – Effect of Leak Time to 90% of Target Inspiratory Pressure Ferreira JC at al, Chest 2009
Summary: NIV for Acute Care • Main Indications – COPD, CHF, Immunocompromised • Data accumulating for others – Asthma, Hypoxemic (Trauma), Extub Failure • Technological advances – New masks, ventilators • Proper application techniques, monitoring and skilled staff still important