Download
1 / 43
450 likes | 775 Views
Bone and Joint Infections. February 13, 2003 Cass Djurfors. Objectives:. Osteomyelitis Septic Arthritis Epidemiology Clinical features Diagnosis Management. Epidemiology. Bimodal age distribution Under 20 Over 50 Pediatrics: boys>girls Usually no identifiable risk factors Adults:

E N D
Bone and Joint Infections February 13, 2003 Cass Djurfors
Objectives: • Osteomyelitis • Septic Arthritis • Epidemiology • Clinical features • Diagnosis • Management
Epidemiology • Bimodal age distribution • Under 20 • Over 50 • Pediatrics: • boys>girls • Usually no identifiable risk factors • Adults: • Usually have risk factors
Bone and Joint Infections: Mechanism • Hematogenous seeding most common • Seeding from a contiguous source of infection • Direct inoculation of the bone, from surgery, trauma or joint aspiration
Risk factors for bone and joint infections: • diabetes mellitus • sickle cell disease • AIDS • alcoholism • IV drug abuse • chronic corticosteroid use • preexisting joint disease • other immunosuppressed states • postsurgical patients—especially those with prosthetic devices
Pathogens: • Bacteria are most common • Viruses, fungi and parasites are possible • Staph aureus most common in all ages except neonates • GBS most common in neonates • H. influenzae b has essentially disappeared as a pathogen in vaccinated children
Pathogens: • Gonococcal arthritis is the most common type of septic arthritis in individuals under 30 years old • In the elderly, gram-negative bacteria account for a higher percentage of cases of bone and joint infections than in younger people • MRSA, MRSE, and VRE have emerged as a significant microbiologic problem in the past decade
Pathogens: • Usually unimicrobial • Polymicrobial (36 to 50%) more likely in diabetic foot osteomyelitis, posttraumatic osteomyelitis, chronic osteomyelitis, and chronic septic arthritis
Osteomyelitis: Presentation • May be acute or chronic • Pain over the affected bone • In children: limp or refusal to weight • Localized warmth, swelling, and erythema • Fever is inconsistently present • Systemic complaints often reported: headache, fatigue, malaise, and anorexia
Osteomyelitis: Presentation • Point tenderness over the infected segment • Palpable warmth and soft-tissue swelling with erythema may be present
Osteomyelitis: Diagnosis • WBC is neither sensitive nor specific • Values commonly range from normal to 15,000/mm3 • ESR usually elevated • One series reported 90% sensitivity • Very nonspecific however • Can be used to follow treatment • CRP • yet another nonspecific marker of inflammation
Osteomyelitis: Diagnosis • Plain films: • Low sensitivity early in the disease • 3-5 days: may detect soft tissue edema • 7-10 days: >66% still have normal x-rays • 30-50% of bone mineral must be lost to detect lucency on plain film • By 28 days, >90% of plain films will be positive • Characteristic finding: lucent lytic lesions of cortical bone destruction • Advanced disease: lytic lesions are surrounded by dense, sclerotic bone, and sequestra may be noted
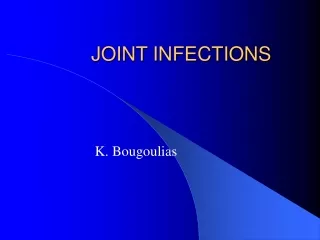
Plain radiograph of tibia. Lucent areas in metaphysis are sites of advanced osteomyelitis
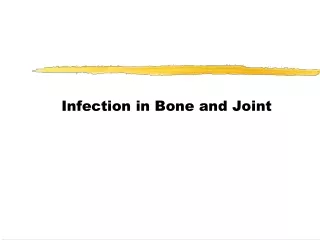
Plain radiograph of humerus. Distal portion of humerus has involucrum formation, representing advanced case of osteomyelitis.
Osteomyelitis: Diagnosis • Bone Scan: • More useful early on than plain radiographs • Can detect osteomyelitis within 48 to 72 hours of disease onset • Sensitivity 90% with technetium-99 scan • False positive rate as high as 64% • Trauma, surgery, tumours, soft tissue infection
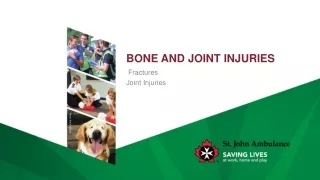
Example of gallium (top) and technetium (bottom) bone scans in advanced osteomyelitis of tibial metaphysis. Both scans show increased radionuclide uptake.
Osteomyelitis: Diagnosis • 111 In-labeled WBC scan • Can distinguish infected bone from bone that has increased turnover from fractures, surgery, prostheses, osteoarthropathy, and tumor • Usually reserved for situations of equivocal or normal bone scans in patients where osteomyelitis is still a consideration
Osteomyelitis: Diagnosis • CT • Used for infection in bones that are difficult to visualize on plain radiographs and bone scans: sternum, vertebrae, pelvic bones, and calcaneus • Appears as rarefaction, or lucent areas, on the CT scan images • Gas may also be visible in bony abscess cavities • Limitation: disease must be present for > 1 week
Osteomyelitis: Diagnosis • MRI • Good for early detection • Limited availability
Osteomyelitis: Diagnosis • Microbiologic Diagnosis: • Needle aspiration or surgical specimen is best • Swab of draining wound or sinus is not adequate • Blood cultures in untreated patients are positive ~50% of the time
Differential Diagnosis: • Tumour: • Osteoid osteoma, chondroblastoma, Ewing’s sarcoma, metastases, lymphoma • Trauma • Myositis ossificans • Erythema nodosum • Cellulitis • Eosinophilic granuloma
Osteomyelitis: Management • IV Antibiotics • Empiric broad spectrum initially • Narrow appropriately when sensitivities available • 4-6 weeks • +/- Surgical debridement • Often not needed for acute hematogenous osteomyelitis in children • Required in the diabetic foot or chronic osteomyelitis • HBO • Controversial
Special considerations • Kids: usually acute hematogenous and often responds to Abx alone • Vertebral osteomyelitis • Risk of paralysis! • Watch for epidural abscess • Careful with back pain and fever in IVDU • Post-traumatic osteomyelitis: • 10% of open fractures • 2% with puncture wounds: Pseudomonas aeruginosa and S. aureus
Special considerations • Diabetic foot: • Usually chronic and polymicrobial • Surgical debridement almost always required • Amputation often required • Sickle cell disease: • Increased risk of osteomyelitis • S. aureus and Salmonella species
Disposition: • Inpatient • Outpatient IV antibiotic therapy • Outpatient PO antibiotic therapy (usually as step-down)
Septic Arthritis: Presentation • Usually hematogenous but may also result from contiguous spread or direct inoculation • Occurs in all age groups • Most common in children • Usually monoarticular • Polyarticular in less than 10% of pediatric cases and less than 20% of adult cases • Hip and knee are most frequently affected
Septic Arthritis: Presentation • Predisposing factors: • Any joint disease • Osteoarthritis • Gout • Rheumatoid arthritis • Surgery • IVDU
Septic Arthritis: Presentation • Usually acute in onset • Joint pain is main feature – worse with movement (careful with immunosuppressed and steroid dependent patients) • Kids may refuse to use the affected limb • Fever - 80% of children, > 40% of adults
Septic Arthritis: Presentation • Physical exam: • Joint is held in position of greatest comfort, slight flexion • Swelling, erythema, and warmth in almost all cases • Palpation of the septic joint causes exquisite pain • Both flexion and extension of the joint cause severe pain • Effusion
Septic Arthritis: Diagnosis • Joint fluid for culture and analysis • Knee joint is both the most likely to be infected and the easiest to aspirate in the ED • Other joints (hip) may require ortho consultation +/- ultrasound or fluoroscopy-guided aspiration • Iatrogenic septic arthritis occurs in less than 1 in 10,000 joint injections or aspirations
Septic Arthritis: Diagnosis • Joint fluid: • aerobes, anaerobes and fungi • Gram stain • Cell count and differential - wbc > 50000/mm3 • Glucose – decreased in septic arthritis with joint fluid/serum glucose ratio < 1:2. • Synovial tissue from arthroscopy can be helpful in diagnosis
Septic Arthritis: Diagnosis • Blood cultures positive in 25% to 50% of cases • ESR elevated in ~90% • WBC may or may not be elevated • Plain radiographs not very helpful except to reveal joint effusion • Bone scan will be “hot” but causes unnecessary delay
Special Considerations: • Kids: • More common than osteomyelitis • Of all cases in kiddies, 2/3 under age 2 • Neonates: GBS, S. aureus, GNB • >3 months: S. aureus > GAS > S. pneumo • Teenagers and young adults: • N. gonorrhoeae • Most are symptomatic with genital/oral infection • Classic triad of disseminated gonococcal infection is migratory polyarthritis, tenosynovitis, and dermatitis • Joint fluid may be negative…treat on suspicion
Septic Arthritis: Differential • Kids • Osteomyelitis • JRA • Transient synovitis • Legg-Calvé-Perthes disease • Slipped capital femoral epiphysis • Rheumatic fever
Septic Arthritis: Differential • Adults: • Osteomyelitis • Gout • Pseudogout • Reiter’s syndrome • Psoriatic arthritis • Arthritis associated with inflammatory bowel disease and ankylosing spondylitis • Traumatic hemarthrosis
Septic Arthritis: Management • Orthopedic emergency • Immediate IV Abx • Needle vs. surgical decompression • Abx alone in gonococcal arthritis only
Septic Arthritis: Disposition • Diagnostic joint fluid aspirate or high clinical suspicion requires admission • Non-diagnostic aspirates with equivocal clinical findings may be discharged home and re-evaluated in 24 hours • Be conservative (consider admission) for patients with joint disease, prosthetic joints or immunosuppression and suspected septic arthritis