Download
1 / 90
940 likes | 1.26k Views
SECOND HEART SOUND Dr SHAJUDEEN .K DM Cardiology Resident Calicut Medical college. History. “S2 is the key to auscultation ” : Aubrey Leathem

E N D
SECOND HEART SOUND Dr SHAJUDEEN .K DM Cardiology Resident Calicut Medical college
History • “S2 is the key to auscultation” : Aubrey Leathem • Respiratory variation first described by Potain (1866) • Term “Hangout interval” coined by shaver laboratory.
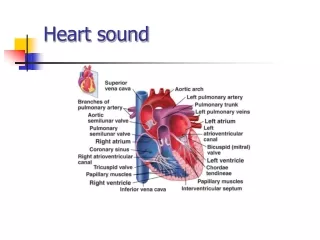
Genesis of S2 • During systole blood flow from LV to Aorta & RV to PA. Once pressure in the great vessels becomes more than corresponding ventricle and hang out interval is over, blood flow reverses , this retrograde flow is stopped suddenly by semilunar valves when the elastic limits of the tensed leaflets are met during closure of valves
This causes vibrations in the cardiohemic system. High frequency generated from this vibration is the Second heart sound.
Hang out interval • It is the time interval from the crossover of the pressure between RV and PA or LV and Aortaduring the ejection phase of systoleto the actual closure of the Pulmonary or Aortic valve respectively.
Cardiac cycle recorded by high fidelity catheter tipped manometer
Normal values of Hangout intervals • Pulmonary circulation: 43-86 msec • Systemic circulation :< 15msec • iePulmonary hangout interval >Systemic
Factors influencing the duration of Hangout interval • Pressure in the arteries • Vascular resistance • Compliance of Vessels
Aorta is a higher pressure and less compliant vessel so hangout interval of aortic is less than the pulmonary side • Pulmonary circulation is Low pressure ,low resistance, high capacitance circulation .So hang out interval more
Reasons for Higher frequency S2 compared to S1 • The tautness of the semilunar valves more compared to A-V valves. • The Greater elastic coefficient of the taut arterial walls that provide the principal vibrating chambers for the second sound,in comparison with the much looser, less elastic ventricular chambers that provide the vibrating system for the first heart sound.
Why S2 duration shorter than S1? • Normally duration of S1 is 0.14 second and S2 is 0.11 second . • The reason is that, semilunar valves are more taut than the A-V valves, so they vibrate for a shorter time than do the A-V valves.
Normal S2 EXPIRATION (Split < 30msec) INSPIRATION (Split > 30msec)
Why P2 Delayed? • RV systolic ejection last longer than LV ejection even though RV and LV Mechanical systole has same duration • This occurs due to prolonged hangout interval of pulmonary circulation.
Why A2 is earlier and louder than P2 • Due to High Diastolic pressure gradient acoss the aortic valve • When compared to pulmonary circulation, LV ejection time is small as aortic hangout interval is less
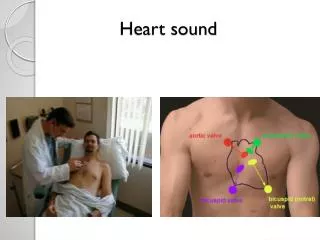
Clinical Examination Of s2 • At 2nd to 3rd Left ICS preferably with Diaphram of the stethescope. • Spliting best apreciated at second Left intercostal space.
Clinical examination of S2 Two important Points to observe while examining for S2 are. • Splitting of S2 • Intensity of each component of S2
Normal Splitting of S2 EXPIRATION (Split < 30msec) INSPIRATION (Split > 30msec)
Normal splitting of S2 Normal A2 P2 interval During expiration : < 30 msec During inspiration : 40-50 ms Splitting occurs because of delayed P2 (73%) and early A2 (27%).
Factors affecting normal splitting of S2 • Age : As age increases split duration decreases. Single S2 during both phases of respiration is a normal finding in subjects with age >40yrs • Depth of respiration • Position of body : In recumbent position prominent splitting in both phases of respiration is a normal finding
Recent views regarding inspiratory widening of split • Complex interplay of dynamic changes in pulmonary vascular impedenceand changes in pulmonary and systemic venous return. Net effect is prolonged RV ejection and a concomittent decrease in LV ejection causing widening of split in inspiration.
Inspiration causes more negative intrathoracicpressure 1) Increased venous return 2) Increase capacitance of the pulmonary vessels Pulmonary hang out interval increases & RV ejection time increases Decreased pulmonary venous flow to the left atrium. So LV ejection time decreases so A2 occurs early So A2 P2 interval > 30 msec
Abnormal splitting can be either absent/inaudible split (single S2) or presence of audible expiratory splitting both in supine and upright position
Abnormal Splitting of S2 includes • Persistent physiological split • Wide fixed split of S2 • Reverse split of S2 • Narrow Physiological split with Loud P2 • No Split : ie Single S2 Expiratory split interval> 30msec
Wide physiological splitting important mechanism • Delayed P2 Delayed electrical activation of RV Prolonged RV mechanical systole Increased Pulmonary Hang out interval • Early A2 Shortened LV mechanical systole
Delayed electrical activation of RV • Complete RBBB • LV ectopic beat • LV pacing
Prolonged RV mechanical systole • Moderate to severe PS with intact IVS • Right heart failure • Acute Massive pulmonary embolism • Anomalous venous connection to RA
Increased Hangout interval • Mild Pulmonary stenosis • Idiopathic dilatation of pulmonary artery • Normotensive ASD • Unexplained audible expiratory splitting in normal subjects
Shortened LV mechanical systole • Severe Mitral Regurgitation • Moderate to Large VSD
Wide fixed splitting A2 P2 widely split and split remains fixed ie remains unchanged during respiration or valsalva
Wide : Due to delay in P2 because of increased pulmonary vascular capacitance prolonging the hangout interval and increased RV ejection time
Fixed : As little or no change in RV filling and stroke volume during inspiration .so little or no inspiratory delay occurs to P2
Causes of wide fixed split • Moderate to Large OstiumSecundum ASD • Severe right heart failure
Reverse or paradoxical splitting splitting • S2 Split>30msec during expiration with reversal of sequence ie P2-A2 • Presence of reverse splitting always indicate significant underlying Heart disease • Almost all cases of reversed split are due to dalayed A2
Types of Reversed split • Type 1 or classic : Only this type is audible clinically • Type 2 Detected Phonographically • Type 3
Type 1 Reversed split No split during inspiration. But splitting during expiration with reverse sequence due to delay in A2 It occurs due to delayed LV Electro mechanical systole
Type 2 or Partially Reversed splitting of S2 • Normal Inspiratory splitting But Expiratory splitting • of S2 with Reverse sequence • It resemble wide fixed split.But during expiration • sequence of sound is P2-A2
Type 3 Reversed splitting of S2 ie similar to type 2 but difference is that A2 P2 and P2-A2 seperation is ≤30 ms and so S2 is heard as a single sound in both phase of respiration
Clinical recognition of Reversed split of S2 • Trace the two components of S2 to the apex.If the second component of S2 is tracable up to apex , reverse split present. • (normally only first component of S2(ie A2) is tracable up to apex, And second component is heard only at pulonaryarea.In reverse split A2 is the second component.)
Clinical recognition of Reversed split of S2 • Valsalva testing
Differentiation of P2-A2 in reversed Split • Auscultate from pulmonary area to apex concentrating on the two components of S2. The component which disappears at apex is the pulmonary component.