Download
1 / 53
530 likes | 554 Views
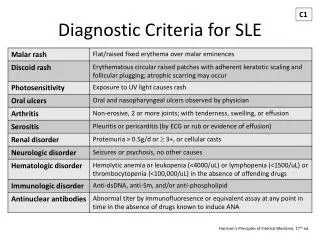
Guideline for SLE management. 高雄長庚醫院風濕過敏免疫科. Epidemiology of SLE. Subacute Cutaneous Lupus Erythematosus. Table 61-1. FREQUENCY OF CLINICAL SYMPTOMS IN SLE AT ANY TIME. Table 9-3. THE SPECTRUM OF ANAs. CAUSES OF POSITIVE ANTINUCLEAR ANTIBODIES. Serological Tests to Aid Diagnosis of SLE.

E N D
Guideline for SLE management 高雄長庚醫院風濕過敏免疫科
Table 61-1. FREQUENCY OF CLINICAL SYMPTOMS IN SLE AT ANY TIME
Main patterns of autoantibody • Homogenous:Anti-histone • Peripheral:Anti-dsDNA, Anti-lamine • Speckled :A large family of nonhiston antigens • -Coarse:Anti-Sm, Anti-U1-nRNP • -Fine:Anti-Ro, Anti-La • -Distinct speckles varying in number(PBC) • Anti-p80-coilin, Anti-p95 • Nucleolar :Scleroderma or overlap syndrome • DNA topoisomerase:nucleolar speckles • PM-Scl:homogenous decorating nucleoli • Fibrillarin (U3-RNP):clummy nucleolar • NOR-90:nucleolar speckles • Centromere :CREST syndrome, and PBC • Cytoplasmic :ANCA,
ANA Negative Positive Peripheral (rim) Centromere Nucleoli Diffuse (honogeneous) No disease Lab error Treatment Remission Antigen XS Nephrotic syndrome Anti-dsDNA Histone Raynaud’s phenomenon Scleroderma Anti-nucleoprotein SLE SLE RA Drug LE SLE RA Drug LE CREST Sdleroderma Speckled RNP Sm RO (SS-A) La PcNA Scl-70 PM/Jo/Ku/Mi No specificity UCTD SLE RA Liver disease Mono Any chronic inflammatory disease SLE SLE SLE SLE Scleroderma PM/DM SLE MCTD RA Scleroderma UCTD Sogren’s syndrome Sogren’s syndrome
Primary Respiratory System Involvement in Systemic Lupus Erythematosus
Pulmonary Involvement In SLE • Pleural disease • Acute lupus pneumonitis • Chronic interstitial lung disease • Pulmonary hemorrhage • Pulmonary embolism • Pulmonary vascular disease • Diaphragmatic dysfunction
Characteristic Clinicopathologic Correlations in the Major Classes of Lupus Nephritis
Morphological Classification of Lupus Nephritis (modified WHO Classification)
INDICES OF ACTIVITY AND CHRONICITY IN LUPUS NEPHRITIS* *Individual lesions are scored 0 to 3+ (absent, mild, moderate, severe). Indices are composite scores for individual lesions in each category of activity or chronicity. Necrosis/karyorrhexis and cellular crescents are weighted by a factor of 2.
SLE and ESRD (1) • 5-22% of SLE patients progress to ESRD requiring H/D • In USA, Iupus nephropathy accounting for 1.4% off all ESRD • Decreased clinical and serological lupus activity following ESRD. Some theories had: • 1.Depressed cellular and humoral immunity • 2.Lack of mediators produced by the kidney • 3.Removal of lupus factors by dialysis itself • 4.Nature end point in SLE • Survival of lupus patients on dialysis versus non-SLE dialysis patients:no significant
SLE and ESRD (2) • Renal transplant graft survival of lupus versus non-lupus patients:no difference • Lupus patients have slightly better outcome with LR rather than CAD grafts • The transplantation time following dialysis need at least 3 months • Recurrence of transplanted allograft is often similar to histologic or immunofluorescent type as in the origin kidney, but it is a rare event.
NEUROPSYCHIATRIC MANIFESTATIONS IN SYSTEMIC LUPUS ERYTHEMATOSUS
PATHOGENETIC MECHANISMS CAUSING NEUROPSYCHIATRIC SYMPTOMS IN SYSTEMIC LUPUS ERYTHEMATOSUS
Pathogenesis of Neuropsychiatric Events in Patients with SLE † Intrathecal production or entrance through a blood-brain barrier disturbed by vascular injury.
FREQUENCY OF ABNORMAL LABORATORY TESTS COMMONLY USED IN THE EVALUATION OF NEUROPSYCHIATRIC LUPUS ERYTHEMATOSUS
Proactive and preventive strategies in addition to lupus therapies(1) • Patients education programs, eliminate patient nonadherence • Monitor vital signs, update physical examination, and have laboratory work done • Adhere to a general conditioning exercise program to minimize osteoporosis and muscle atrophy • Cognitive therapy for lupus “fog”;biofeedback for Raynaud’s phenomenon • Counseling and stress management • Physical and occupational therapy, ergonomic work station evaluation
Proactive and preventive strategies in addition to lupus therapies(2) • Aggressive proactive management of blood pressure, blood sugars, serum lipids, and weight. Smoking cessation. • Yearly bone densitometry and osteoporosis prevention measures. • Annual electrocardiogram and chest x-ray • Prompt evaluation of all fevers • Periodic screening with carotid duplex scanning, treadmill, or stress testing; screening for, and prophylactic management of, antiphospholipid antibodies.
Therapies for lupus patients with skin lesions(1) • General • Avoid sun: clothing, sunscreens, avoid hot part of day with most UV-B light, camouflage cosmetics • Stop smoking (so antimalarials works better) • Thiazides and sulfonylureals may exacerbate skin disease
Therapies for lupus patients with skin lesions(2) • Routine therapy • Topical steroids, intralesional steroids • Hydroxychloroquine • Oral corticosteroids • Dapsone for bullous lesions
Therapies for lupus patients with skin lesions(3) • Advanced therapy for resistant causes • Subacute cutaneous lupus: mycophenylate mofetil, retinoids, or cyclosporine • Discoid lesions: chloroquine, clofazimine, thalidomide, or cyclosporine • Lupus profundus: dapsone • Chronic lesions over 50% of body: topical nitrogen mustard, BCNU, or tacrolimus • Vasculitis: may need immunosuppressives
Therapy for lupus patients with arthritis(no internal organ involvement) • First line: NSAIDs • Cyclooxygenase-2 specific inhibitors (but may induce thrombotic risk in patients with antiphospholipid antibodies) • Low dose hydroxychloroquine(200mg twice a day)
Indications of high dose corticosteroid therapy in lupus patients • Severe lupus nephritis • CNS lupus with severe manifestations • Autoimmune thrombocytopenia with extremely low platelet counts (e.g.<30000/mm3) • Autoimmune hemolytic anemia • Acute pneumonitis caused by SLE. • Others: severe vasculitis with visceral organ involvement, serious complications from serositis (pleuritis, pericarditis, or peritonitis)
Life-Threatening Manifestations of SLE: Responses to glucocorticoids(1) • Manifestations often responsive to glucocorticoids • Vasculitis • Severe dermatitis of subacute cutaneous lupus erythematosus or SLE • Polyarthritis • Polyserositis—pericarditis, pleurisy, peritonitis • Myocarditis • Lupus pneumonitis
Life-Threatening Manifestations of SLE: Responses to glucocorticoids(2) ~(continue) • Glomerulonephritis—proliferative forms • Hemolytic anemia • Thrombocytopenia • Diffuse CNS syndrome—acute confusional state, demyelinating syndromes, intractable headache • Serious cognitive defects • Myelopathies • Peripheral neuropathies • Lupus crisis—high fever and prostration
Life-Threatening Manifestations of SLE: Responses to glucocorticoids(3) • Manifestations not often responsive to glucocorticoids • Thrombosis—includes strokes • Glomerulonephritis—scarred end-stage renal disease, pure membranous glomerulonephritis • Resistant thrombocytopenia or hemolytic anemia—occurs in a minority of patients; consider splenectomy, cytotoxics, danazol, or cyclosporine/neoral therapies • Psychosis related to conditions other than SLE, such as glucocorticoid therapy
Therapy for patients with lupus nephritis • Previously untreated patients with active lupus nephritis or severe manifestations ( decreased renal function and /or high-grade proteinuria) • First line: high doses of corticosteroids (about 1mg/kg/day) • Cytotoxic drugs or other immunosuppressive drugs
The indications of cytotoxic drugs use in the treatment of lupus nephritis • Active and severe GN despite treatment with high dose prednisone • Responded to corticosteroids but require an unacceptably high dose to maintain a response. • Unacceptable side effects from corticosteroids. • Chronic damage on a renal biopsy and other indicators of a poor prognosis.
Systemic therapies for nonorgan-threatening lupus • Nonsteroidal anti-inflammatory drugs • Antimalarials • Thalidomide • Hormonal interventions: dehydroepiandrosterone, testosterone patches, bromocriptine, prolactin • Immunosuppressive therapies: azathioprine, methotrexate, leflunomide
The management of organ-threatening lupus • Existing immunosuppressive therapies: cyclophosphamide, mycophenolate mofetil, cyclosporine A, fludarabine, cladribine (2-CDA) • Apheresis • Intravenous immunoglobulin • Various biologic agents: BlyS inhibitor, CTLA-4Ig, LL2IgG • Stem cell transplantation
Use of Cytotoxic Drugs in SLE : Azathioprine • requires 6–12 months to work well • 1–3 mg/kg/day(initial dose) • 1–2 mg/kg/day(maintenance dose) • Advantage:probably reduces flares, reduces renal scarring, reduces glucocorticoid dose requirement • Side effects: Bone marrow suppression, leukopenia, infection(herpes zoster), infertility, malignancy, early menopause, hepatic damage, nausea
Use of Cytotoxic Drugs in SLE: Cyclophosphamide • requires 2–16 weeks to work well • Initial dose:1-3 mg/kg/day orally or 8–20 mg/kg intravenously once a month plus mesna • Maintenance dose:0.5–2 mg/kg/day orally or 8–20mg/kg intravenously every 4–12 wks plus mesna • Adverse effects:probably reduces flares, reduces renal scarring, reduces glucocorticoid dose requirement • Adverse effects: marrow suppression, leukopenia, infection, infertility, malignancy, menopause,cystitis,nausea
The treatment in lupus patients with autoimmune thrombocytopenia • Splenectomy • Danazol • Immunosuppressive or cytotoxic drugs: azathioprine, cyclophosphamide • Intravenous immunoglobulin(IVIG)