Download
1 / 56
560 likes | 575 Views
STRESS ECHO. DEEPAK NANDAN. Stress echo is a family of examinations in which 2D echocardiographic monitoring is undertaken before , during & after cardiovascular stress Cardiovascular stress exercise pharmacological agents. PHYSIOLOGY.

E N D
STRESS ECHO DEEPAK NANDAN
Stress echo is a family of examinations in which 2D echocardiographic monitoring is undertaken before , during & after cardiovascular stress • Cardiovascular stress exercise pharmacological agents
PHYSIOLOGY • Coronary blood flow – pulsatile & phasic • Precapillary arterioles – resistance vessels * principal contributor of resistance * main controller of coronary blood flow • ↑ CBF on ↑ demand occurs through reduction in resistance at this level
CORONARY BLOOD FLOW RESERVE • Maximal CBF / basal CBF • Magnitude of bf ↑ secondary to any stress relative to resting flow • In discrete stenosis – CFR begins to ↓ when stenosis reaches 50% dm • CFR is abolished when stenosis reaches 90% • Resting bf remains constant up to 85- 90% of the stenosis
Cellular Mechanism of Ischemia • Consequence(s) of Mechanical Dysfunction • Mechanical Dysfunction • Abnormal Contraction and Relaxation • Diastolic Tension • Diastolic Wall Tension (Stiffness) Extravascular Compression Blood Flow to Microcirculation ( O2 delivery to Myocytes) O2 Consumption (to maintain tonic contraction) ATP Hydrolysis O2 Demand O2 Supply Modified from: Belardinelli et al. Eur Heart 8 (Suppl. A):A10-A13, 2006
BASIC PRINCIPLES OF STRESS ECHO • ↑ Cardiac work load - ↑O2 demands- demand supply mismatch- ischemia • Impairment of myocardial thickening and endocardial motion
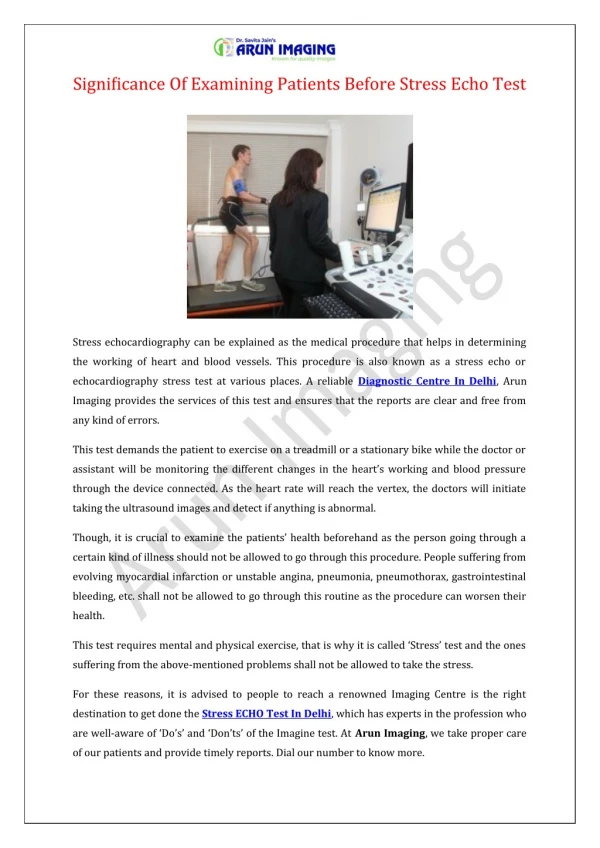
Treadmill vs supine bicycle advantage • Add information • Wide spread availability • Simple protocol • High work load • > Sensitive Disadvantage • Imaging post ex only Advantage • Image through out the exercise- peak • Onset of RWMA • Better image quality • Contrast stress echo • > Specific Disadvantage • Lower work load • Supine position affects ex.physio
Information obtained from Exercise Stress but not available with Pharmacological Test • Exercise Duration/Tolerance • Reproducibility of Symptoms with Activity • Heart rate response to exercise • Blood Pressure response • Detection of Stress Induced Arrhythmias • Assess control of angina with medical therapy • Prognosis
Indication pharmacological stress echocardiography • Inadequate exercise • Left bundle branch block • Paced ventricular rhythm • pre-excitation or conduction abnormality • Medication: beta-blocker, calcium channel blocker • Evaluation of patients very early after MI(<3 days) or • angioplasty stent(<2weeks) • Poor image degradation with exercise • Poor patient motivation to exercise
Pharmacologic Stress Agents Inotropic agents Dobutamine Arbutamine Coronary vasodilator Dipyridamole Adenosine Stress agents
DOBUTAMINE STRESS ECHO • Dobutamine- synthetic catecholamine • Inotropic & chronotropic- β1,β2 & α • Action: onset – 2 min half life – 2 min: continous IV • Metabolizd by cathechol-o-methyl transferase • Excretion: hepatobiliary system and kidney
Works by inducing myocardial ischemia • Modest ↑ SBP and ↓DBP • May be arrhythmogenic (0.7% rate in 8500 consecutive studies performed at Mayo Clinic) • Usually ineffective in patients on beta blockers • High rate of side effects • Hypotension induced does not have prognostic value unlike TMT • Does not interact with dipyridamole
Dipyridamole Potent coronary vasodilator Provoke anginal attack in angina patients Vasodilation effect inhibition of reuptake of adenosine by the endothelial cell CBF increases 4 to 5 times in normal vessel Reduction of subendocardial blood flow in stenotic coronary artery
Dipyridamole Coronary steal phenomenon Standard protocol: 0.54 mg/kg for 4 min High dose protocol: 0.84mg/kg Antidote: theophylline
Dipyridamole Contraindication active wheezing high degree AV block hypotension(SBP<90 mmHg) recent use of dipyridamole(<24 hours) Relative contraindication Hx of reactive airway disease sick sinus syndrome severe sinus bradycardia
Adenosine Naturally occuringagent Types of receptors A1: slowing HR and conduction A2a: c-AMP – decrease calcium uptake by SR -- smooth muscle relaxation vasodilation Half life: 2 seconds need constant IV infusion Rapidly removed from RBC and endothelial cell
Adenosine – side effect Flushng: 37% Dyspnea: 35% GI discomfort: 15% Headache:14% Light-headedness 9% Most side effect – short-lived and mild
Myocardial contrast in stress echo • Left vent opacification for border enhancement • Myocardial perfusion imaging • Perfusion at resting state-stress is performed and perfusion imaging is done at peak stress
Stress Echo Stress Echocardiography Diagnosis Prognosis Viability Treatment
Exercise –preferred-add information • > sensitive in CAD compared to dobutamine • Treadmill >sensitive, Bicycle>specific • Bicycle –during stress-> accurate presence and extend of disvs pat choice,availability etc. • Dobutamine is limited to pats who cant exert adequately & when the Q of viability is addressed • In pharmaclogical stress dobutamine is the agent- produces true ischemia than a flow mismatch
INTERPRETATION OF STRESS ECHO • Subjective assessment of regional wall motion • Compares wall thickening & endocardial excursion at baseline and stress • Limitation- subjective & nonquantitative • Measures like EF, ESV change, and strain rate to overcome limitations
Strain rate-myocardial velocity gradient -postsystolic shortening • TDI/Strain imaging> sensitive • Ischemia delays onset & rate of regional myo relaxation • Time quantified using TDI • QRS-onset of relaxation-350-400ms • Interval↓ by 34+/_10% in nl segments in response to high dose dopamine • ↓in interval is <12+/-18% in ischemic seg
Grade 1-normal 2-hypokinesis 3-akinesis 4-dyskinesis • Nl WMSI-1 at baseline and stress • Any score>1-abnormal • Good prognostic value
Hypokinesia-<5 mm of endocardial excursion • Akinesis - -vesyst thickening & endo excursion • Dyskinesis –systolic thinning & outward motion • nlresp-hyperkinesis • Absence –low work load, β blockade, cardiomyopathy & delayed post stress imaging • Localisation>specific in multivessel dis & in LAD than RCA/LCX
Prognostic value A new wall motion abnormality,rest & exercise WMSI,ESV response-correlated with risk
Prognostic value of stress echo • Independent predictors of cardiac events a)WMSI with exercise b) ST ↓≥1 mm c) treadmill time • Risk Index(RI)=1.02(WMSI)+1.04(ST change)− 0.14(Treadmilltime) • RI in upper quartile(+0.66 to+2.02)– risk was highest(30%) • Prognostic value is comparable in women and men
PRE-OPERATIVE RISK STRATIFICATION WITH DOBUTAMINE STRESS ECHO *Mayo Clinic, 530 Patients
Perioperative marker of coronary event • patients with a positive electrocardiographic response to treadmill stress test but no inducible wall motion abnormality on stress echocardiogram have a very low rate of adverse cardiovascular events during follow-up
VIABILITY OF MYOCARDIUM • That has the potential for functional recovery;- either stunned/hibernating myocardium • >6mm thickness -viable segment • Stunned or hibernating improved contractility with dobutamine , not in infarcted myocardium • Biphasic response – low dose ↑contractility(10 to 20 mcg/kg), at higher dose CBF ↓-- contractility ↓
Biphasic response is the most predictive of the functional recovery after revascularisation • Sustained improvement/no change-nonviable • For viability assessment – nuclear techniques are more sensitive dobut stress echo more specific PPV-similar NPV- favoursdobut stress echo