Download
1 / 63
641 likes | 824 Views
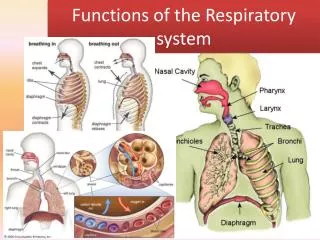
Structures and Functions of the Respiratory System. Gas Exchange. Ventilation Diffusion (alveolar-capillary membrane) Perfusion Diffusion (capillary-cellular level). Ventilation Movement of Chest Wall. Ventilation. Depends on volume and pressure changes within thoracic cavity

E N D
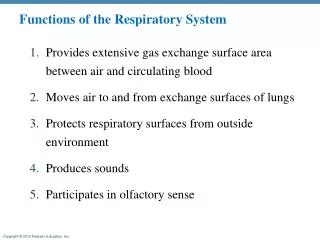
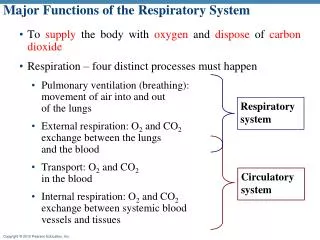
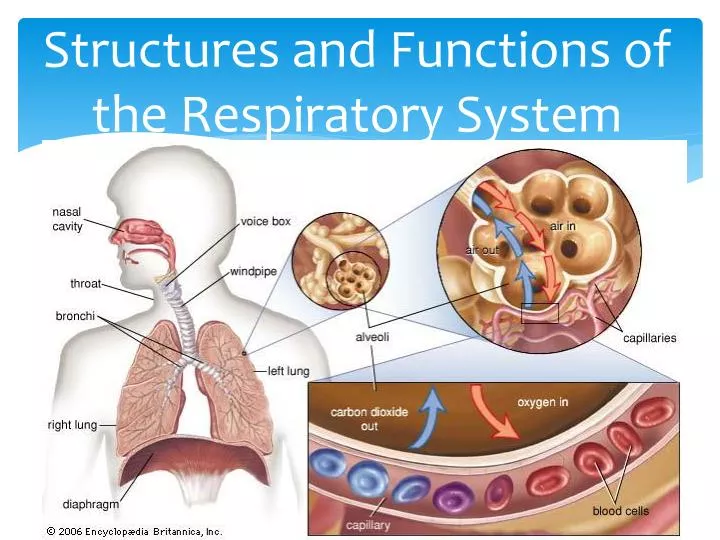
Gas Exchange Ventilation Diffusion (alveolar-capillary membrane) Perfusion Diffusion (capillary-cellular level)
Ventilation • Depends on volume and pressure changes within thoracic cavity • Diaphragm is major muscle of inspiration; also external intercostal muscles. Contraction increases diameter of thoracic cavity→ ↓ intrathoracic pressure →air flows into respiratory system • Expiration is passive process d/t lung elasticity. ↑ intrathoracic pressure→ air flows out of lungs • Accessory muscles
Control of Ventilation Neural control- respiratory center in medulla & pons Central chemoreceptors – sensitive to pH Peripheral chemoreceptors- sensitive to paO2 Patients with COPD- hypoxic drive WOB- amount of effort required for the maintenance of a given level of ventilation (as WOB ↑s, more energy is expended for adequate ventilation)
Factors Influencing Ventilation • Airway resistance- opposition to gas flow • Compliance- distensibility / stretchability - Dependent on lung elasticity & elastic recoil of chest wall - Decreased compliance- lungs difficult to inflate - Increased compliance- destruction of alveolar walls & loss of tissue elasticity
Ventilation-Perfusion • Adequate diffusion depends on balanced ventilation-perfusion (V/Q) ratio • Normal lung: V=4L/min; Q= 5L/min (0.8) • If imbalanced: gas exchange interrupted - High V/Q= “wasted” or dead-space ventilation - Low V/Q= blood “shunted” past area; no gas exchange occurs
COPD • Progressive, irreversible airflow limitation • Associated with abnormal inflammatory response of lungs to noxious particles or gases
COPDEtiology Cigarette smoking Occupational chemicals and dusts Air pollution Infection Heredity- A1-antitrysin deficiency Aging
COPDPathophysiology Primary process is inflammation Inhalation of noxious particles→ inflammatory cells release mediators (leukotrienes, interleukins, TNF) → airways become inflammed with increased goblet cells → excess mucus production (bronchitis) & structural remodeling to peripheral airways with ↑d collagen & scar tissue
COPDPathophysiology Destruction of lung tissue caused by imbalance of proteinases/antiproteinases results in emphysema with loss of attachments & peripheral airway collapse (Centrilobar- affects respiratory bronchioles/upper lobes/mild disease; panlobar- alveolar ducts, sacs, respiratory bronchioles- lower lobes/AAT deficiency
COPDPathophysiology Air goes into lungs easily but unable to come out; air trapped in distal alveoli, causing hyperinflation & overdistension PV thickens with ↓surface area for gas exchange- V/Q mismatch
COPDBehaviors • Develop slowly around 50 years of age after history of smoking • Cough, sputum production, dyspnea • In late stages, dyspnea at rest • Wheezing/chest tightness- may vary • Prolonged I:E, ↓BS, tripod position, pursed-lip breathing, edema • ↑ A-P diameter of chest • Advanced- weight loss, anorexia (hypermetabolic state) • Hypoxemia, possible hypercapnia • Bluish-red color from polycythemia, cyanosis
COPDDiagnosis PFTs (↑ RV, ↓FEV1) CXR ABGs Sputum C&S if infection suspected EKG- RV hypertrophy 6 minute oxy-walk
COPDComplications Cor pulmonale- RV hypertrophy 2º pulmonary hypertension (late) Exacerbations of COPD Acute respiratory failure Peptic ulcer and gastroesophageal reflux disease Depression/anxiety
COPD- Collaborative Care Smoking cessation Medications- bronchodilators (inhaled & step-wise), Spriva (LA anticholinergic), ICS Oxygen therapy RT- PLB, diphragmatic, cough, CPT, nebulization therapy Nutrition- Avoid over/underweight, rest 30” before eating, 6 small meals, avoid foods that need a great deal of chewing, avoid exercise 1 hr before meal, take fluids between meals to avoid stomach distension
COPDNursing Diagnoses Ineffective Breathing Pattern Impaired Gas Exchange Ineffective Airway Clearance Imbalanced Nutrition: Less than Body Requirements
Asthma • Chronic inflammatory disorder associated with airway hyperresponsiveness leading to recurrent episodes (attacks) • Often reversible airflow limitation • Prevalence increasing in many countries, especially in children
AsthmaPathophysiology Airway hyperresponsiveness as a result of inflammatory process Airflow limitation leads to hyperventilation Decreased perfusion & ventilation of alveoli leads to V/Q mismatch Untreated inflammation can lead to LT damage that is irreversible Chronic inflammation results in airway remodeling
AsthmaPotential Triggers Allergens – 40% Exercise (EIA) Air pollutants Occupational factors Respiratory infections – viral Chronic sinus and nose problems Drugs and food additives – ASA, NSAIDs, ß-blockers, ACEi, dye, sulfiting agents Gastroesophageal reflux disease (GERD) Psychological factors- stress
Asthma Inflammation – Effects Bronchospasm Plasma exudation Mucus secretion AHR Structural changes
Asthma InflammationClinical Manifestations Cough Chest tightness Wheeze Dyspnea Expiration prolonged -1:3 or 1:4, due to bronchospasm, edema, and mucus Feeling of suffocation- upright or slightly bent forward using accessory muscles Behaviors of hypoxemia- restlessness, anxiety, ↑HR & BP, PP
AsthmaDiagnosis • History and patterns of symptoms • Measurements of lung function • PFTs- usually WNL between attacks; ↓ FVC, FEV1 • PEFR- correlates with FEV • Measurement of airway responsiveness • CXR • ABGs • Allergy testing (skin, IgE)
AsthmaTherapeutic Goals • No (or minimal)* daytime symptoms • No limitations of activity • No nocturnal symptoms • No (or minimal) need for rescue medication • Avoid adverse effects from asthma medications • Normal lung function • No exacerbation • Prevent asthma mortality • * Minimal = twice or less per week
AsthmaCollaborative Management Suppress inflammation Reverse inflammation Treat bronchoconstriction Stop exposure to risk factors that sensitized the airway
AsthmaMedications • AntiinflammatoryAgents • Corticosteroids- suppress inflammatory response. Reduce bronchial hyperresponsiveness & mucus production, ↑ B2 receptors • Inhaled – preferred route to minimize systemic side effects • Teaching • Monitor for oral candidiasis • Systemic – many systemic effects – monitor blood glucose • Mast cell stabilizers- NSAID ; inhibit release of mediators from mast cells & suppress other inflammatory cells (Intal, Tilade)
AsthmaMedications • Antiinflammatory Agents • Leukotriene modifiers • Block action of leukotrienes • Accolate, Singulair, Zyflo) • Not for acute asthma attacks • Monclonal Ab to IgE • ↓ circulating IgE • Prevents IgE from attaching to mast cells, thus preventing the release of chemical mediators • For asthma not controlled by corticosteroids • Xolair SQ
AsthmaMedications • Bronchodilators • B-agonists- SA for acute bronchospasm & to prevent exercised induced asthma (EIA) (Proventil, Alupent); LA for LT control • Combination ICS + LA B-agonist (Advair) • Methylxanthines- Theophylline: alternative bronchodilator if other agents ineffective. Narrow margin of safety & high incidence of interaction with other medications • Anticholinergics- block bronchoconstriction . Additive effect with B-agonists (Atrovent)
AsthmaPatient Teaching- Medications • Name/dosage/route/schedule/purpose/SE • Majority administered by inhalation (MDI, DPI, nebulizers) • Spacer + MDI- for poor coordination • Care of MDI- rinse with warm H2O 2x/week • Potential for overuse • Poor adherence with asthma therapy is challenge for LT management • Avoid OTC medications
AsthmaCollaborative Care • GINA- decrease asthma morbidity/mortality & improve the management of asthma worldwide • Education is cornerstone • Mild Intermittent/Persistent: avoid triggers, premedicate before exercise, SA or LA Beta agonists, ICS, leukotriene blockers • Acute episode: Oxygen to keep O2Sat>90%, ABGs, MDI B-agonist; if severe- anticholinergic nebulized w/B agonist, systemic corticosteroids
AsthmaNursing Diagnoses Ineffective Airway Clearance Impaired Gas Exchange Anxiety Deficient Knowledge
Pneumonia HAP- pneumonia occurring 48 hours or longer after admission VAP- pneumonia occurring 48-72 hours after ET intubation HCAP- hospitalized for 2 or more days within 90 days of infection; resided in LTC facility; received IV therapy or wound care within past 30 days of current infection; attended a hospital or dialysis clinic Aspiration pneumonia- abnormal entry of secretions into lower airway
PneumoniaPathophysiology • Congestion • Fluid enters alveoli; organisms multiply & infection spreads • Red hapatization • Massive capillary vasodilation; alveoli filled with organisms, neutrophils, RBCs, & fibrin • Gray hepatization • Blood flow decreases & leukocytes & fibrin consolidate in affected part • Resolution • Resolution & healing; exudate processed by macrophages
PneumoniaRisk Factors • Aging • Air pollution • Altered LOC • Altered oral normal flora secondary to antibiotics • Prolonged immobility • Chronic diseases • Debilitating illness • Immunocompromised state • Inhalation or aspiration of noxious substances • NG tube feedings • Malnutrition • Resident of Long-term care • Smoking • Tracheal intubation • Upper respiratory tract infection
Pneumonia Behaviors Usually sudden onset Fever, shaking chills, SOB, cough w/purulent sputum, pleuritic CP Elderly/debilitated- confusion or stupor
Pneumonia- Complications Pleuritis Pleural effusion- 40% of hospitalized patients Atelectasis Bacteremia Lung abscess Empyema Pericarditis