Download
1 / 62
620 likes | 814 Views
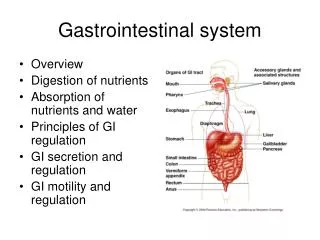
Highlights of the developing gastrointestinal system. Saliva newborns produce little saliva until 3-4 months of age Sucking and extrusion reflex until 3-4 months Stomach increases to 200-300 by 12 months Immature muscle tone of lower esophageal sphincter and low capacity of the stomach

E N D
Highlights of the developing gastrointestinal system • Saliva • newborns produce little saliva until 3-4 months of age • Sucking and extrusion reflex until 3-4 months • Stomach • increases to 200-300 by 12 months • Immature muscle tone of lower esophageal sphincter and low capacity of the stomach • Deficient digest enzymes lead to gas, diarrhea sensitization for food allergies and microscopic hemorrhages
Highlights of the developing gastrointestinal system • Intestinal • Infants vulnerable to GI infections due to lower intestinal flora and reduced stomach acidity • Breast milk increases flora and provides some protection • Myelination of nerves to anal sphincter matures at about age two
Highlights of the developing gastrointestinal system • Liver • Immature at birth resulting in inefficient detoxifying of substance and medications • Slow development of glycogen storage capacity during early infancy • Other • Infants are more prone to dehydration and fluid and electrolyte imbalances due to greater body surface area, high rate of metabolism and immature kidney function
Credits • The previous slides on the highlight of the developing GI system and the next slide on abdomen assessment tips are credited to: Pediatric Nursing Made Incredibly Easy BY: Lippincott Williams and Wilkins
Abdomen assessment tips • Warm hands • Note guarding when child is moving around • Flex knees to relax muscles • Deep breathing or distraction • Use child’s hands to “help” with the exam • Auscultate before palpation
Esophageal AtresiaTracheoesophageal Fistula • Basic terminology • Esophagus: tube that connects the mouth to the stomach • Trachea: "windpipe" • Atresia: absence of a normal opening • Congenital: found at birth • Fistula: abnormal passage from a body organ to the body surface or between two internal body organs. Taken from Texas Pediatric Surgery Associates @ http://www.pedisurg.com/PtEduc/TEF-Esophageal_Atresia.htm
Esophageal AtresiaType A • Both segments of the esophagus end in blind pouches. Neither segment of esophagus is attached to the trachea.
Tracheal Esophageal FistulaType B • The upper segment of the esophagus forms a fistula to the trachea (TEF). The lower segment of the esophagus ends in a blind pouch (EA). This is a very rare form of EA/TEF.
TEF Type C • The upper segment of the esophagus ends in a blind pouch (EA). The lower segment of the esophagus is attached to the trachea (TEF). This is the most common type of EA/TEF.
TEF Type D • Both segments of the esophagus are attached to the trachea. This is the rarest form of EA/TEF.
TEF Type E • There is no esophageal atresia as the esophagus is continuous to the stomach. However, fistula is present between the esophagus and the trachea.
Credits • The last five slides were taken from the EA/TEF Child and Family Support connection at: • http://www.eatef.org/description.html
Manifestations of EA/TEF • Prenatal polyhydraminos • Vomiting or choking on first feeding • Appearance of drooling in infancy • Frothy saliva in mouth • Abdominal distension • Aspiration pneumonia
Nursing Care for EA/TEF • Assessment of newborn first feeding • Place any infant with symptoms on NPO • Suction to clear the airway • Gastrostomy tube to decompress stomach • Head elevated • IV • Antibiotics • Oxygen • Note that bag/mask ventilation may cause gastric distention if a distal fistula is present
An important emotional need • Make sure these infants are provided with sucking to satisfy this most important need and to avoid “oral aversion”
Associated Congenital Defects • Cardiac • Gastrointestinal • Genitourinary • Musculoskeletal
Additional Credits to: • DWAYNE C. CLARK, MD, LCDR, MC, USNR; Esophageal Atresia and Tracheoesophageal Fistula. American Family Physician. Feb 15, 1999.
Imperforate Anus The tissues between the GI tract and anus are separated Ranges from stenosis to complete separation to failure of the anus to form GI tract may form a fistula to GU tract
Imperforate AnusManifestations • Patency of anus checked at birth by taking a rectal temperature. All temperatures afterwards are axillary. • Failure to pass meconium in the first 24 hours
Imperforate AnusNursing Measures • NPO and prepared for surgery • High type defects require a colostomy and anal repair at a later date. • Anal repair requires post operative dilatation of the new anus (to improve muscle tone and prevent narrowing) will begin in the hospital and continue for some months. Stool softeners and a high-residue diet will need to continue throughout childhood.
Credits • Hebe Molmenti, M.D., Ph.D • Medline Plus • http://www.nlm.nih.gov/medlineplus/ency/presentations/100030_4.htm
Pyloric Stenosis • Pyloric Stenosis (narrowing) is an obstruction at the lower end of the stomach (pylorus) caused by an overgrowth (hypertrophy) of the circular muscles of the pylorus or by spasms of the sphincter
Pyloric Stenosis Diagram of normal stomach and pylorus. Note the cross-section showing normal pyloric opening
Pyloric Stenosis • Diagram of stomach with pyloric stenosis. Note the cross-section showing how the pyloric opening is very narrowed.
Pyloric Stenosis Post Surgery • Diagram of stomach after repair of pyloric stenosis. Note (in the cross-section) how an incision has been made in the muscle, enlarging the pylorus and relieving the obstruction
Credits • The last three slides on pyloric Stenosis are from the website of Texas Pediatric Surgical Associates • http://www.pedisurg.com/PtEduc/Pyloric_Stenosis.htm
Manifestations of Pyloric Stenosis • Symptoms begin at 2 to 3 weeks • Projectile vomiting • Constantly hungry and will eat immediately after vomiting • Symptoms of dehydration and malnutrition • Olive shaped mass in Right Upper Quadrant
Nursing Care • Care for dehydration and electrolyte imbalances • NPO; prepare for surgery
Post operative CarePyloric Stenosis • Progress feeding from oral electrolyte solution to formula or breast milk • I/O; daily weights • Provide for suck need • Incision clean and dry • Frequent burping • Elevated and on right side after feeding • Pain management
Celiac Disease • Known as gluten enteropathy or celiac sprue; results in mal-absorption • Autoimmune response to gluten, a type of protein found in wheat, barley, rye and to a lesser extent oats • Immune system attacks and damages the villi that normally absorb nutrients
Clinical Manifestations of Celiac • Bulky, frothy, foul smelling stool • Fatty stools (steatorrhea) • Diarrhea or constipation • Weight loss/failure to thrive • Anemia • Anorexia • Coagulation difficulties and vitamin deficiencies • Pot belly and muscle wasting
Diagnosis of Celiac • Immunoglobulin A (IgA) • anti-tissue transglutaminase (tTGA) • IgA anti-endomysium antibodies (AEA)
Wheat, Barley, Rye, Oats Durum Couscous Semolina Spelt Kamut Bulgur Triticale Malt Hydrolyzed Vegetable protein (HVP) Hydrolyzed Plant Protein (HPP) MCG products Some vegetable cooking sprays Some medications Some cosmetics Treatment of CeliacGluten Free Diet
Credits on Celiac Disease • http://digestive.niddk.nih.gov/ddiseases/pubs/celiac/ • Elliot, David MD @http://www.uihealthcare.com/news/currents/vol4issue2/celiacdiseae.html • National Foundation for Celiac Awareness
Hirschsprung’s Disease • Absence of ganglionic innervation to the muscle of a segment of the bowel, usually in the lower portion of the sigmoid colon. This results in a lack of normal peristalsis
Hirschsprung’s DiseaseClinical Manifestations • Failure to pass meconium in the first 24 to 48 hours • Abdominal distention and palpable stool masses • Ribbon like stools • Anorexia, vomiting, failure to thrive • Bile stained or fecal vomiting
Hirschsprung’s Disease Nursing Care • Pre-surgery may need enemas; remember normal saline enemas to prevent water intoxication! • Post op care: • IV fluids, I/O, wound care • Possible ostomy care • No rectal thermometer or suppositories • Oral feedings once bowel sounds begin • Continence of stool may be delayed in these kids, advise parents accordingly
Intussusception • The slipping of one part of the intestine into another part just below it, usually seen at the ileocecal valve. The slipping is often referred to as telescoping.
Intussusceptionclinical manifestations • Pain: loud cries, straining efforts, kicking and drawing of the legs towards abdomen • Bilious vomits • Currant jelly stools from blood and mucous • Fever • Possible signs of shock • A very rigid abdomen • Sausage shaped mass in the RUQ
IntussusceptionPost operative Nursing Care • IV • Antibiotics • I/O • Incision Care; possible colostomy care • Monitor Bowel Sounds • Pain management
Meckel’s diverticulum • Small duct that fails to disappear during fetal life usually near the ileocecal valve; a small pouch is formed. • Manifested by painless bleeding from the rectum and sometimes abdominal pain • May progress to hemorrhage, inflammation, obstruction. • Treated by surgery
Inguinal Hernia • Protrusion of part of the abdominal contents through the inguinal canal in the groin • May be: • Reducible • Incarcerated • Strangulated