Download
1 / 30
650 likes | 2.21k Views
ATOPIC DERMATITIS. Clinical Course and Therapeutic Options. Bindi M. Nikhar, M.D., FAAP Division of Dermatologic and Dental Drug Products, ODE V. Introduction. Atopic dermatitis is a chronic inflammatory disease of the skin primarily seen in the pediatric age group

E N D
ATOPIC DERMATITIS Clinical Course and Therapeutic Options Bindi M. Nikhar, M.D., FAAP Division of Dermatologic and Dental Drug Products, ODE V
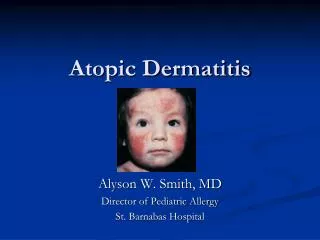
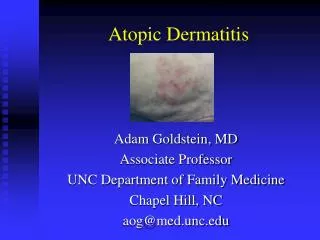
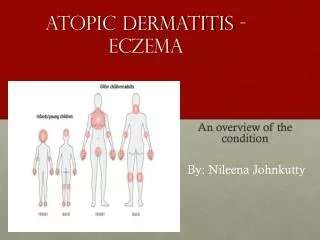
Introduction • Atopic dermatitis is a chronic inflammatory disease of the skin primarily seen in the pediatric age group • Characterized by dry skin, pruritus, erythema, edema, scaling, excoriations, oozing, lichenification • Increasing prevalence, rising costs • Together with asthma and allergic rhinitis forms part of the ‘atopic triad’
Epidemiology • 10-20% of children in industrialized countries develop atopic dermatitis • Rising incidence, commoner in higher socioeconomic groups • Overall clearance 50-60%. 80% of children with severe disease continue to have lifelong exacerbations.
Morbidity Impact on quality of life occurs at all ages. • Psychological problems from visible skin lesions due to stigmatization • Itch-scratch cycle • Sleeplessness, lack of concentration at school or work • Repeated treatments, time involved, financial costs
Cost • Drain on financial resources of patients and health services • Costs increase with disease severity, highest in first few years • While FDA does not consider pharmacoeconomic issues in drug approvals, we recognize that cost is an important factor in drug availability.
Clinical Manifestations • Seen in early infancy, in 50 - 75% of cases, age of onset is 6 months or younger • Clearance rate of 60% expected by age 16, relapses occur in adulthood • Worse prognosis – severe childhood disease, early onset, concomitant or family history of asthma/allergic rhinitis, biparental history of atopy
Clinical Features • Three main age-related stages. Dry skin and pruritus associated with all stages. Skin barrier function decreased, may lead to increased absorption of topically applied treatments. Usually improves with adequate treatment
Clinical Phases • Infantile Phase ( 0-2 years ) Onset around 3 months of age. Under 6 months, the face and scalp commonly involved, at an older age, limb folds and hands involved Red, scaly, crusted weeping patches with excoriations seen on both cheeks and extensor surfaces of extremities Course chronically relapsing and remitting
Clinical Phases (cont’d) • Childhood Phase ( 2-12 years ) Papular areas in flexural regions common. Persistent rubbing and scratching leads to lichenified plaques and excoriations • Adult Phase (puberty onwards) Flexural lichenified eczema with facial involvement in periorbital regions seen. Upper trunk, shoulders, scalp affected with chronic remissions and exacerbations
Reported Immunological Features of Atopic Dermatitis • Increased IgE production • Specific IgE to multiple antigens • Increased basophil spontaneous histamine release • Decreased CD8 suppressor/cytotoxic number and function • Increased expression of CD 23 on mononuclear cells • Chronic macrophage activation with increased secretion of GM-CSF, PGE2 and IL-10 • Expansion of IL-4 and IL-5 secreting Th 2-like cells • Decreased numbers of IFN-gamma-secreting Th 1-like cells
Diagnosis of Atopic Dermatitis • This requires the presence of three or more major and three or more minor criteria as defined by Hanifin and Rajka • Major criteria • Pruritus • Lichenification • Chronic or chronically relapsing course • Personal or family history of atopy Minor criteria There are 23 minor criteria
Management of Atopic Dermatitis • No single, ideal treatment available • Each patient should have a flexible plan tailored for their need • Dietary history important, dietary manipulation controversial • Family education important • Reduce exposure to allergens
General Treatment Guidelines • Moisturizers – are the cornerstone of therapy in AD. Frequent use important because AD is often accompanied by dry skin. Creams, ointments or lotions can be used depending on individual needs • Avoidance of drying bathing products • Itch control – Distressing symptom, use oral antihistamines, try to break the itch-scratch cycle
General Treatment Guidelines (cont’d.) • Control of infection – Patients with extensive AD are often colonized with Staph. aureus. A course of oral antibiotics ± topical antibiotics needed for lichenified, excoriated lesions not responding to treatment. Viral infections, eg. warts, eczema herpeticum are seen in these patients
Selection of treatment This depends on • Disease severity • Age • Compliance • Efficacy • Safety data • Treatment costs
Rx Treatment Options • Topical corticosteroids • Topical immunosuppressants • Systemic corticosteroids Off-Label and other treatment options • Photochemotherapy • Cyclosporin • Azathioprine • Thymopentin • Interferon-γ therapy • Traditional Chinese medicine • γ -linoleic acid
Topical corticosteroids (TCS) • First introduced in the 1950s and are currently the mainstay of prescription therapy for atopic dermatitis • Safe and effective when used as recommended • Weakest steroid that will keep the eczema under control should be used • Potent steroids should be used in short pulses, generally 2-3 weeks
Factors to consider when prescribing topical corticosteroids • Type of preparation (base and potency) – Base can be ointment, cream, emulsion, gel or lotion Potency classified from group I (most potent) to VII (least potent) • Acute or chronic eczema • Age of child • Site to be treated • Extent of eczema • Method of application
Mechanism of action of TCS 1. Antiinflammatory effects TCS affect inflammatory cells, chemical mediators and tissue responses which are all responsible for cutaneous inflammation 2. Antiproliferative effects TCS may reduce mitotic activity in the epidermis, leading to flattening of the basal cell layer and thinning of the stratum corneum and stratum granulosum
Mechanism of action of TCS (cont’d) 3. Atrophogenic Effects TCS can promote atrophy of the dermis through inhibition of fibroblast proliferation, migration, chemotaxis and protein synthesis
Systemic Effects of TCS • If a TCS is absorbed percutaneously in significant quantities, it can cause systemic adverse side effects similar to systemically administered corticosteroids. Discussed under adverse effects
Adverse effects of TCS Can result from • the drug substance, or • the vehicle which can potentiate problems
Systemic adverse effects of TCS • Suppression of hypothalamic-pituitary-adrenal axis • Iatrogenic Cushing’s syndrome • Growth retardation in infants and children These effects are usually associated with the large body surface area use of potent TCS.
Risk factors for systemic adverse effects • Young age (infants and children) • Liver and renal disease • Amount of TCS applied • Extent of skin disease treated • Frequency of application • Length of treatment • Potency of drug • Use of occlusion It is not established whether catch up growth in children will occur when TCS are discontinued.
Local side effects of TCS • Epidermal Atrophy - wrinkled skin with prominent vasculature, pseudoscars, striae or purpura • Steroid dependence/rebound • Glaucoma/cataracts • Increased susceptibility to bacterial, fungal and viral infections
Topical Immunosuppressants • Newest pharmacological class for AD • Introduced in this decade • Direct immunosuppressive action in diseases with immunologic basis • 2 FDA approved products • Tacrolimus (FK506) (trade name Protopic) • Pimecrolimus (SDZ ASM 981) (trade name Elidel)
Background • Protopic (tacrolimus) ointment approved on 12/08/2000, 0.03% ointment approved for children 2 to 15 years, 0.1% ointment approved for adults. • Indication in both age groups is short and intermittent long term therapy of patients with moderate to severe AD. • Systemic tacrolimus (Prograf) first introduced for prevention of allograft rejection, now used in kidney, liver and heart transplantation
Background (cont’d) • Elidel (pimecrolimus) cream 1% approved on 12/13/2001 • Indicated for patients 2 years of age and older for short and intermittent long term therapy in the treatment of mild to moderate atopic dermatitis • Both drugs not approved for use in children less than 2 years of age • Systemic absorption can take place in both adult and pediatric age groups from topical application of both drugs
Background (cont’d.) • Pediatric patients enrolled in clinical studies of tacrolimus and pimecrolimus had an increased incidence of certain adverse events eg. viral infections compared to vehicle. • Currently, the effects of topical immunosuppressants on the developing immune system are unknown
Indications for use (Second-line) • Both Protopic and Elidel are indicated for patients in whom the use of alternative, conventional therapies are deemed inadvisable because of potential risks, or in the treatment of patients who are not adequately responsive to or are intolerant of alternative, conventional therapies