Download
1 / 135
1.9k likes | 3.13k Views
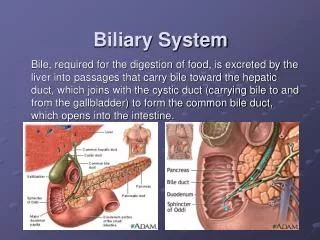
The Pathology of Liver & Biliary System Part-1. Is life worth living? It depends on the liver!. This is liver !. I f individual hepatocytes are destroyed but the architecture of the lobule is not destroyed, the remaining hepatocytes will totally regenerate the liver parenchyma.

E N D
The Pathology ofLiver & Biliary SystemPart-1 Is life worth living? It depends on the liver!
This is liver ! • If individual hepatocytes are destroyed but the architecture of the lobule is not destroyed, the remaining hepatocytes will totally regenerate the liver parenchyma. • The Greek titan Prometheus had his liver devoured each day by a monster bird (simurg), but it always grew right back.
Belongs to RE & Digestive system. • Hemopoietic organ before birth. • 1500 g, (2.5% of body weight) right hypochondrium, wedge shape • end-stage cirrhotic 700 g liver, • an alcoholic 7000 g liver • Center of metabolic homeostasis. • Portal and Hepatic blood supply. • Micro-architecture – Lobules / Acini.
Lobule acinus 3 2 1
Zones of a lobulus: • Zone 1 is the hepatocytes near the portal areas, • Zone 2 is the hepatocytes midway between the portal areas and central veins, • Zone 3 is the hepatocytes around the central veins.
Functions • Metabolism – Carbohydrate, Fat & Protein • Secretory – Bile, Bile acids, salts & pigments • Excretory – Bilirubin, drugs, toxins • Synthesis – Albumin, coagulation factors • Storage – Vitamins, carbohydrates etc. • Detoxification – Toxins, ammonia, etc.
Acute Liver Disorder: Viral, Drug, Gall stones, alcohol toxicity. Chronic Liver Disease: Chronic hepatitis, Cirrhosis, viral, alcohol, Autoimmune hepatitis. Congenital Disorders: Haemochromatosis, Wilsons, 1AT deficiency Tumors: Benign: Adenoma, angioma, Nodular hyperplasia Malignant: Hepatocellular carcinoma, Cholangiocarcinoma, Hepatoblastoma, Angiosarcoma. Cysts: Simple, Hydatid. Disorders
Circulatory Disorders • Liver Infarction • Portal Vein Obstruction and Thrombosis • Passive Congestion and Centrilobular Necrosis • Peliosis Hepatis • Hepatic Vein Thrombosis (Budd-Chiari Syndrome) • Veno-Occlusive Disease
Liver Infarction • Liver infarcts are rare(double blood supply) • Cause is thrombosis or compression of an intrahepatic branch of the hepatic artery by • embolism, • neoplasia, • polyarteritis nodosa, • sepsis. • Zahn infarct:Occlusion of an intrahepatic branch of the portal vein (does not cause ischemic infarction) sharply demarcated area of red-blue discoloration infarct of Zahn (old terminology). • In this condition, there is no necrosis, only marked stasis in distended sinusoids, with secondary hepatocellular atrophy.
Infarcts are uncommon because the liver has two blood supplies-portal venous system and hepatic arterial system. The infarcts seen here are yellow, with geographic borders and surrounding hyperemia. About half of liver infarcts occur with arteritis, and the remaining half are due to a variety of causes
Portal Vein Obstruction and Thrombosis Extrahepatic causes of portal vein obstruction include: • (1) massive enlargement of hilar lymph nodes owing to metastatic abdominal cancer; • (2) phlebitis resulting from peritoneal sepsis (e.g., acute diverticulitis or appendicitis); • (3) splenic vein thrombosis secondary to pancreatitis; • (4) post-surgical thrombosis following upper abdominal procedures. The most common intrahepatic cause: • Cirrhosis of the liver.
Banti’s syndrome: • splenomegaly, • hypersplenism, • portal hypertension • Postulated causes: • neonatal omphalitis, • dehydration, • sepsis, • umbilical vein catheterization, • hypercoagulable myeloproliferative disorders, • biliary tract surgery, • peritonitis, • exposure to arsenicals.
Passive Congestion • Acute and chronic passive congestion of the liver usually reflects cardiac decompensation most commonly right-sided failure • Liver: • slightly enlarged, • tense, • cyanotic, with rounded edges. • On cut section, • there is an excessive ooze of blood, • centrilobular areas are soft, • surrounded by paler, fatty liver substance in the portal areas (the “nutmeg liver”).
"nutmeg" liver seen with chronic passive congestion of the liver. Note the dark red congested regions that represent accumulation of RBC's in centrilobular regions
Nutmeg:Fruit of nutmeg tree Myristica fragrans. This tree grows in the Molucca Islands and elsewhere in Indonesia
Centrilobular Necrosis • Left-sided cardiac failure or shock hepatic hypoperfusion and hypoxia ischemic necrosis of hepatocytes in the central region of the lobule (Centrilobular necrosis) macroscopically as a slight depression of necrotic lobular centers. • Microscopy: • sharp demarcation of viable and necrotic hepatocytes moving from portal tract to the centrilobular region. • The necrosis is coagulative, • there is no inflammation.
Cardiac cirrhosis • Chronic severe congestive heart failure fibrosis of the liver increased venous pressure centrilobular hypoxia. • Centrilobular liver fibrosis is distinctive.
If chronic hepatic passive congestion continues for a long time, a condition called "cardiac cirrhosis" may develop in which there is fibrosis bridging between central zonal regions, as shown below, so that the portal tracts appear to be in the center of the reorganized lobule. This process is best termed "cardiac sclerosis" because, unlike a true cirrhosis, there is minimal nodular regeneration
Peliosis Hepatis • Sinusoidal dilation • Although peliosis may be associated with hepatomegaly and even hepatic failure, it is more commonly a lesion found incidentally. • Etiology: • Drugs • anabolic steroids • oral contraceptives • danazol.
Two types have been described. In one, the parenchymal variant, there are cystic spaces filled with blood and without an endothelial lining.
In the other, the phlebectatic variant, the prominent vascular spaces are in continuity with what appears to be dilated sinusoids
Hepatic vein thrombosis ("Budd-Chiari") • Common causes: • polycythemia vera • hypercoagulable blood • invasion of the hepatic veins by hepatocellular carcinoma. • Complications: • ascites, • venous infarction.
Portal Hypertension • Increased resistance to portal blood flow • prehepatic, intrahepatic, and posthepatic causes. Prehepatic portal hypertension • Obstructive thrombosis and narrowing of the portal vein before it ramifies within the liver • massive splenomegaly shunts excessive blood into the splenic vein, which drains into the portal vein.
Intrahepatic portal hypertension • cirrhosis, • schistosomiasis • veno-occlusive disease • massive fatty change • diffuse fibrosing granulomatous disease, (sarcoidosis, miliary tuberculosis) • diseases affecting the portal microcirculation.
Posthepatic portal hypertension • severe right-sided heart failure, • constrictive pericarditis, • hepatic vein outflow obstruction.
Consequences of Portal hypertension • Ascites, • The formation of portosystemic venous shunts, • Congestive splenomegaly, • Hepatic encephalopathy.
Hemolytic jaundice too much bilirubin beingproduced Hemolytic anemias Intravascular hemolysis Extravascular hemolysis Big hematomas GI bleeding Red infarcts Ineffective erytopoiesis Thalassemias Megaloblastic anemias Hepatocellular jaundice liver fails to uptake and/or conjugate bilirubin Newborns Hypoperfusion Bad alcoholism Genetic deficiency of bilirubin UGT activity (Crigler-Najhar syndrome) Gilbert Syndrome (mixed-etiology) Diffuse hepatocellular disease (e.g. Viral or drug-induced hepatitis, cirrhosis) Jaundice (icterus)increased bilirubin in the bloodstream !!! The serum unconjugated bilirubin will be elevated!!!
Cholestatic jaundice liver doesn't send bilirubin to the right place Problems with the liver cells drugs (estrogen, anabolic steroids) Dubin-Johnson (pigmented) disease Rotor (non-pigmented) disease Byler's disease benign familial recurrent intrahepatic cholestasis hepatitis, cirrhosis, alcoholism Problems with the bile ducts in the liver Biliary cirrhosis Biliary atresia Alagille's syndrome Problems with the bile ducts beyond the liver Gallstones Cancer (biliary, pancreatic, ampullary) Iatrogenic (i.e., the surgeon nicked the common bile duct). !!!The serum conjugated bilirubin will be elevated!!!
Post Hepatic (Obstructive) jaundice • Stone, tumor • Conjugated/Direct, High colored urine, Pre Hepatic (Acholuric) jaundice • Hemolytic • Unconjugated/Indirect, pale urine Hepatocellular jaundice • Viral, alcohol, toxins, drugs • Unconjugated : Liver damage • Conjugated: Swelling, canalicular obstruction
Cholestasis • Hepatocellular dysfunction or intra or extrahepatic biliary obstruction may also present with jaundance. • Characteristic finding: elevated serum Alkaline phosphatase. • Elevated plasma bile acids results with pruritis. • Skin Xanthomas (focal accumulation of cholesterol) • Malabsorbtion of fat soluble vitamins due to reduced bile flow.
Byler Disease: • Progressive intrahepatic cholestasis • Aut. Rec. • This inherited condition results from impairment of bile salts or phospholipid secretion. Making correct diagnosis of the cause of jaundence and cholestatsis is urgent!
Before specific disease processes are discussed general aspects of liver disease and definitions of general morphologic patterns of hepatic injury are reviewed!
jaundice hypoalbuminemia ascites edema hypocholesterolemia coagulopathy(diminished hepatic synthesis of factors II, V, VII,IX, and X). hyperammonemia fetor hepaticus palmar erythema, spider angiomas, gynecomastia & testicular atrophy, enlargement of the parotid glands (in longstanding liver failure). Clinical Findings in Hepatic Failure
Responses to injurious events Necrosis • Ischemic necrosis: • Poorly stained mummified hepatocytes remain (coagulative necrosis). • Apoptosis (Councilman or acidophyl bodies): • in toxic or immunologically mediated necrosis, • isolated hepatocytes round up to form shrunken, pyknotic, and intensely eosinophilic.
Focal necrosis : Necrosis may be limited to scattered cells within the hepatic lobules • Zonal necrosis :Necrosis may involve particular regions of the lobule • Submassive necrosis :Necrosis may entire lobules • Massive necrosis :Necrosis may involve the whole liver
Focal necrosis viral hepatitis. Zonal Necrosis Centrilobular necrosis (3) ischemic injury drugs toxic chemical reactions. Midzonal necrosis (2) yellow fever. Periportal necrosis (1) phosphorus poisoning eclampsia. Massive necrosis severe chemical drug toxicity viral hepatitis. Geographic necrosis typhoid fever, tularemia, brucellosis, herpesvirus, adenovirus. Abscesses: with disseminated candidal or bacterial infection.
There is extensive hepatocyte necrosis seen here in a case of acetaminophen overdose. The hepatocytes at the right are dead, and those at the left are dying. This pattern can be seen with a variety of hepatotoxins. Acute liver failure leads to hepatic encephalopathy
Hepatic injury Degeneration • Ballooning degeneration: • swollen, edematous appearance clumped cytoplasm • large, clear spaces • Cholestasis: • retained biliary material • diffuse foamy swollen appearance to the hepatocyte (Foamy degeneration) • Accumulation of specific substances in viable hepatocytes:iron, copper, viral particles. • Steatosis: Accumulation of fat droplets within the hepatocytes. (steatosis may be either microvesicular or macrovesicular)
Inflammation • Hepatitis • influx of acute or chronic inflammatory cells into the liver • Inflammation may be secondary to • hepatocellular necrosis, • lymphocytic attack of viable antigen-expressing liver cells. • Granulomatous reactions • foreign bodies, • organisms, • drugs.
Regeneration • hepatocyte proliferation • thickening of the hepatocyte cords • some disorganization of the parenchymal structure. Fibrosis • Response to • inflammation • direct toxic insult to the liver. • Fibrosis may develop • around portal tracts or • the central vein or • directly within the space of Disse. • Continuing fibrosiscirrhosis • the liver is subdivided into nodules of regenerating hepatocytes surrounded by scar tissue.
Disruption of the normal liver architecture by fibrous scars which have resulted from loss of liver cells nodules of "regenerative" liver cells, which represent successful regeneration of the ill-perfused remaining hepatocytes. Largely the result of : alcohol abuse, viral hepatitis, chronic hepatitis, biliary disease, iron overload. CIRRHOSIS
CIRRHOSIS; Itis common end result of many chronic liver disorders. Diffuse disorder of liver characterised by: • Complete loss of normal architecture, • Replaced by extensive fibrosis with, • Regeneratingparenchymalnodules.