Download
1 / 61
620 likes | 816 Views
Unit 4 Part 6 Human Immunodeficiency Virus. Terry Kotrla, MS, MT(ASCP)BB. Introduction. Etiologic agent of Acquired Immunodeficiency Syndrome (AIDS). Discovered independently by Luc Montagnier of France and Robert Gallo of the US in 1983-84. Former names of the virus include:

E N D
Unit 4Part 6 Human Immunodeficiency Virus Terry Kotrla, MS, MT(ASCP)BB
Introduction • Etiologic agent of Acquired Immunodeficiency Syndrome (AIDS). • Discovered independently by Luc Montagnier of France and Robert Gallo of the US in 1983-84. • Former names of the virus include: • Human T cell lymphotrophic virus (HTLV-III) • Lymphadenopathy associated virus (LAV) • AIDS associated retrovirus (ARV)
Introduction • HIV-2 discovered in 1986, antigenically distinct virus endemic in West Africa. • One million people infected in US, 30 million worldwide are infected. • Leading cause of death of men aged 25-44 and 4th leading cause of death of women in this age group in the US. • Reduced mortality resulting from the use of highly active antiretroviral therapies is a major factor contributing to the number of persons in the United States living with HIV disease. • Additionally, more than 56,000 new HIV infections are estimated to occur annually
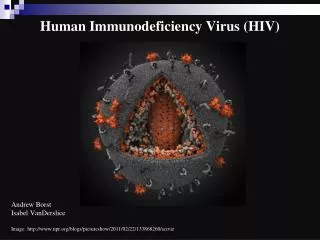
Characteristics of the virus • Icosahedral (20 sided), enveloped virus of the lentivirus subfamily of retroviruses. • Retroviruses transcribe RNA to DNA. • Two viral strands of RNA found in core surrounded by protein outer coat. • Outer envelope contains a lipid matrix within which specific viral glycoproteins are imbedded. • These knob-like structures responsible for binding to target cell.
HIV • The outer shell of the virus is known as the Viral enevlope. • Embedded in the viral envelope is a complex protein known as env which consists of an outer protruding cap glycoprotein (gp) 120, and a stem gp14. • Within the viral envelope is an HIV protein called p17(matrix), and within this is the viral core or capsid, which is made of another viral protein p24(core antigen).
Structural Genes • Three main structural genes: • Group Specific Antigen (Gag) • Envelope (Env) • Polymerase (Pol)
Group Specific Antigen (Gag) • Located in nucelocapsid of virus. • Icosahedryl capsid surrounds the internal nucleic acids made up of p24 andp15. • p17 lies between protein core and envelope and is embedded in the internal portion of the envelope. • Two additional p55 products, p7 and p9, are nucleic acid binding proteins closely associated with the RNA.
Envelope (Env) • Envelope (Env) gene codes for envelope proteins gp160, gp120 and gp41. • These polyproteins will eventually be cleaved by proteases to become HIV envelope glycoproteins gp120 and gp41. • gp160 cleaved to form gp120 and gp41. • gp120 forms the 72 knobs which protrude from outer envelope. • gp41 is a transmembrane glycoprotein antigen that spans the inner and outer membranes and attaches to gp120. • gp120 and gp41 both involved with fusion and attachment of HIV to CD4 antigen on host cells.
Polymerase (Pol) • Polymerase (Pol) codes for p66 and p51 subunits of reverse transcriptase and p31 an endonuclease. • Located in the core, close to nucleic acids. • Responsible for conversion of viral RNA into DNA, integration of DNA into host cell DNA and cleavage of protein precursors.
Viral Replication • http://tinyurl.com/3425m69 • First step, HIV attaches to susceptible host cell. • Site of attachment is the CD4 antigen found on a variety of cells • helper T cells • macrophages • monocytes • B cells • microglial brain cells • intestinal cells • T cells infected later on.
Early Phase HIV Infection • In early phase HIV infection, initial viruses are M-tropic. Their envelope glycoprotein gp120 is able to bind to CD4 molecules and chemokine receptors called CCR5 found on macrophages
Viral Replication • In late phase HIV infection, most of the viruses are T-tropic, having gp120 capable of binding to CD4 and CXCR4 found on T4-lymphocytes.
Viral Replication • The gp120 protein on virus binds specifically to CD4 receptor on host cell with high affinity. • Gp41 causes fusion of the virus to the cell membrane. • After fusion virus particle enters cell. • Viral genome exposed by uncoating particle.
Viral Replication • Reverse transcriptase produces viral DNA from RNA. • Becomes a provirus which integrates into host DNA. • Period of latency occurs.
Viral Replication • After a period of latency lasting up to 10 years viral replication is triggered and occurs at high rate. • CD4 cell may be destroyed in the process, body attempts to replace lost CD4 cells, but over the course of many years body is unable to keep the count at a safe level. • Destruction of large numbers of CD4 cause symptoms of HIV to appear with increased susceptibility to opportunistic infections, disease and malignancy.
Viral Replication • Methods of transmission: • Sexual transmission, presence of STD increases likelihood of transmission. • Exposure to infected blood or blood products. • Use of contaminated clotting factors by hemophiliacs. • Sharing contaminated needles (IV drug users). • Transplantation of infected tissues or organs. • Mother to fetus, perinatal transmission variable, dependent on viral load and mother’s CD 4 count.
Primary HIV Syndrome • Mononucleosis-like, cold or flu-like symptoms may occur 6 to 12 weeks after infection. • lymphadenopathy • fever • rash • headache • Fatigue • diarrhea • sore throat • neurologic manifestations. • no symptoms may be present
Primary HIV Syndrome • Symptoms are relatively nonspecific. • HIV antibody test often negative but becomes positive within 3 to 6 months, this process is known as seroconversion. • Large amount of HIV in the peripheral blood. • Primary HIV can be diagnosed using viral load titer assay or other tests. • Primary HIV syndrome resolves itself and HIV infected person remains asymptomatic for a prolonged period of time, often years.
Clinical Latency Period • HIV continues to reproduce, CD4 count gradually declines from its normal value of 500-1200. • Once CD4 count drops below 500, HIV infected person at risk for opportunistic infections. • The following diseases are predictive of the progression to AIDS: • persistent herpes-zoster infection (shingles) • oral candidiasis (thrush) • oral hairy leukoplakia • Kaposi’s sarcoma (KS)
Oral Hairy Leukoplakia • Being that HIV reduces immunologic activity, the intraoral environment is a prime target for chronic secondary infections and inflammatory processes, including OHL, which is due to the Epstein-Barr virus under immunosuppressed conditions
Kaposi’s sarcoma (KS) • Kaposi’s sarcoma (shown) is a rare cancer of the blood vessels that is associated with HIV. It manifests as bluish-red oval-shaped patches that may eventually become thickened. Lesions may appear singly or in clusters.
AIDS • CD4 count drops below 200 person is considered to have advanced HIV disease • If preventative medications not started the HIV infected person is now at risk for: • Pneumocystis carinii pneumonia (PCP) • cryptococcal meningitis • toxoplasmosis • If CD4 count drops below 50: • Mycobacterium avium • Cytomegalovirus infections • lymphoma • dementia • Most deaths occur with CD4 counts below 50.
Other Opportunistic Infections • Respiratory system • Pneumocystis Carinii Pneumonia (PCP) • Tuberculosis (TB) • Kaposi's Sarcoma (KS) • Gastro-intestinal system • Cryptosporidiosis • Candida • Cytomegolavirus (CMV) • Isosporiasis • Kaposi's Sarcoma • Central/peripheral Nervous system • Cytomegolavirus • Toxoplasmosis • Cryptococcosis • Non Hodgkin's lymphoma • Varicella Zoster • Herpes simplex • Skin • Herpes simple • Kaposi's sarcoma • Varicella Zoster
Infants with HIV • Failure to thrive • Persistent oral candidiasis • Hepatosplenomegaly • Lymphadenopathy • Recurrent diarrhea • Recurrent bacterial infections • Abnormal neurologic findings.
Immunologic Manifestations • Early stage slight depression of CD4 count, few symptoms, temporary. • Window of up to 6 weeks before antibody is detected, by 6 months 95% positive. • During window p24 antigen present, acute viremia and antigenemia.
Immunologic Manifestations • Antibodies produced to all major antigens. • First antibodies detected produced against gag proteins p24 and p55. • Followed by antibody to p51, p120 and gp41 • As disease progresses antibody levels decrease.
Immunologic Manifestations • Immune abnormalities associated with increased viral replication. • Decrease in CD4 cells due to virus budding from cells, fusion of uninfected cells with virally infected cells and apoptosis. • B cells have decreased response to antigens possibly due to blockage of T cell/B cell interaction by binding of viral proteins to CD4 site. • CD8 cells initially increase and may remain elevated. • As HIV infection progresses, CD4 T cells drop resulting in immunosuppression and susceptibility of patient to opportunistic infections. • Death comes due to immuno-incompetence.
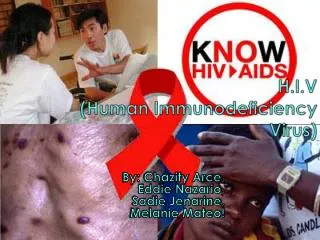
‘typical’ primary HIV-1 infection symptoms symptoms HIV proviral DNA HIV antibodies ‘window’ period HIV viral load HIV-1 p24 antigen 01 2 3 4 5 6 / 2 4 6 8 10 1° infection weeks years Time following infection
Laboratory Diagnosis of HIV Infection • Methods utilized to detect: • Antibody • Antigen • Viral nucleic acid • Virus in culture
ELISA Testing • First serological test developed to detect HIV infection. • Easy to perform. • Easily adapted to batch testing. • Highly sensitive and specific. • Antibodies detected in ELISA include those directed against: p24, gp120, gp160 and gp41, detected first in infection and appear in most individuals
ELISA Testing • ELISA tests useful for: • Screening blood products. • Diagnosing and monitoring patients. • Determining prevalence of infection. • Research investigations.
ELISA Testing • Different types of ELISA techniques used: • indirect • competitive • sandwich • ELISAs are for screening only, false positives do occur and may be due to AI disease, alcoholism, syphilis, and immunoproliferative diseases.
Other Screening Tests • Agglutination tests using latex particles, gelatin particles or microbeads are coated with HIV antigen and will agglutinate in the presence of antibody. • Dot-Blot Testing utilizes paper or nitrocellulose impregnated with antigen, patient serum is filtered through, and anti-antibody is added with enzyme label, color change is positive. • A rapid, cost-effective and may become an alternative to standard ELISA and Western blot testing.
Western Blot • Most popular confirmatory test. • Utilizes a lysate prepared from HIV virus. • The lysate is electrophoresed to separate out the HIV proteins (antigens). • The paper is cut into strips and reacted with test sera. • After incubation and washing anti-antibody tagged with radioisotope or enzyme is added. • Specific bands form where antibody has reacted with different antigens. • Most critical reagent of test is purest quality HIV antigen. • The following antigens must be present: p17, p24, p31, gp41, p51, p55, p66, gp120 and gp160.
Western Blot • Antibodies to p24 and p55 appear earliest but decrease or become undetectable. • Antibodies to gp31, gp41, gp 120, and gp160 appear later but are present throughout all stages of the disease.
Western Blot • Interpretation of results. • No bands, negative. • In order to be interpreted as positive a minimum of 3 bands directed against the following antigens must be present: p24, p31, gp41 or gp120/160. • CDC criteria require 2 bands of the following: p24, gp41 or gp120/160.
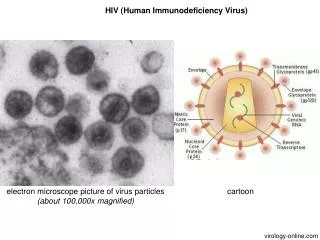
Spectrum of anti-HIV testing early recent / established advanced DNA PCR RNA PCR p24 Ag 3rd gen ELISA 1st gen ELISA Detuned ELISA 1wk 2wk 3wk 2mo 6mo 1yr 2yr 3yr +8yr
Western Blot • Expensive – $ 80 - 100 • technically more difficult • visual interpretation • lack standardisation • - performance • - interpretation • - indeterminate reactions – resolution of ?? • ‘Gold Standard’ for confirmation
Western Blot • Indeterminate results are those samples that produce bands but not enough to be positive, may be due to the following: • prior blood transfusions, even with non-HIV-1 infected blood • prior or current infection with syphilis • prior or current infection with malaria • autoimmune diseases (e.g., diabetes, Grave’s disease, etc) • infection with other human retroviruses • second or subsequent pregnancies in women. • run an alternate HIV confirmatory assay. • Quality control of Western Blot is critical and requires testing with strongly positive, weakly positive and negative controls.
Indirect immunofluorescence • Can be used to detect both virus and antibody to it. • Antibody detected by testing patient serum against antigen applied to a slide, incubated, washed and a fluorescent antibody added. • Virus is detected by fixing patient cells to slide, incubating with antibody.
Detection of p24 HIV antigen • The p24-antigen screening assay is an EIA performed on serum or plasma. • P24 antigen only present for short time, disappears when antibody to p24 appears. • Anti-HIV-1 bound to membrane, incubated with patient serum, second anti-HIV-1 antibody attached to enzyme label is added (sandwich technique), color change occurs. • Optical density measured, standard curve prepared to quantitate results.