Download
1 / 33
340 likes | 453 Views
Celiac sprue. Un caso clinico dal web. Case Presentation. January 1991 J. N. is a 74 year old white female Dx. 12 years ago with irritable bowel syndrome Tx. with Tigan, Lomotil, Donnatal but worsened

E N D
Celiac sprue Un caso clinico dal web
Case Presentation January 1991 • J. N. is a 74 year old white female • Dx. 12 years ago with irritable bowel syndrome • Tx. with Tigan, Lomotil, Donnatal but worsened • Up to 8 loose, watery stools/day; abdominal pain; dec. energy; nausea; and 34 lb. wt. loss in 2 years • Work-up - Upper GI showed hiatal hernia • Pelvic U/S showed small cyst on left ovary
vertigo, iron deficiency anemia Meds: Inderal 20mg Meclizine 25mg wt. 99lb Rectal: no hemorrhoid or mass, +brown stool with mucous, heme - A: IBS P: Metamucil, high fiber diet, Lomotil Case Presentation
Case Presentation November 1991 (9 months later) • Post hysterectomy, 5-6 stools/day despite 8 tabs. Lomotil, Wt. 88 lbs., Abd. - benign, Stool - heme+ • Colonoscopy - Sessile polyp (benign adenoma) • Diverticular disease • EGD - Hiatal hernia and gastritis • Flat appearing duodenal mucosa (villous atrophy and chronic inflammation suggestive of celiac disease)
Case Presentation • Referred to dietitian for gluten-free diet education • Dec. 1991 - Strict diet, asymptomatic, Wt. 86 lbs. • Feels like a “reborn woman” • June 1992 - Strict diet, asymptomatic, Wt. 132 lbs. • June 1993 - Strict diet, asymptomatic, Wt. 141 lbs. • Aug. 1996 - Strict diet, asymptomatic, Wt. 142 lbs
Introduction Key Elements • Evidence of malabsorption • Pathological damage to the small intestine • Response to a gluten-free diet
Etiology and Pathogenesis Environmental Factors • Cereal grains of wheat, rye, barley, and oats • Prolamins = alcohol-soluble proteins of gluten • 12 amino acid segment of the E1b protein of human adenovirus, serotype 12 • 89% of untreated celiac sprue patients • 17% of control subjects
Etiology and Pathogenesis Genetic Factors • 10% prevalence among first-degree relatives • 28-40% concordance rate between HLA identical siblings • 70-75% concordance rate between monozygotic twins • 90% have HLA-B8, HLA-DR3, or HLA-DQw2 haplotype • 25-30% of general population have these haplotypes • Only 0.1% of people with these haplotypes develop celiac sprue
Etiology and Pathogenesis Immunologic Factors • Humoral and cell-mediated mechanisms • Antigliadin antibody triggering the complement cascade • Anti-transglutaminase • Antigliadin antibody causing cytotoxic cell-mediated mucosal damage • Intraepithelial lymphocytes in the absorptive cells producing lymphokines
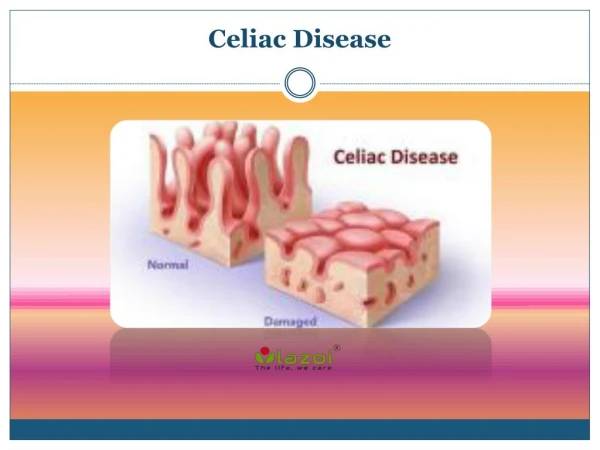
Pathology • Small intestinal mucosa affected (proximal>distal) • Length involved correlates with severity of disease • Villous atrophy and crypt hyperplasia decreasing the villous: crypt ratio • Columnar to cuboidal to squamous absorptive cell • Microvilli decrease • Abnormal tight junctions allow more permeability • Increased mitotic activity
Pathology • Increased numbers of intraepithelial lymphocytes, plasma cells, mast cells, and eosinophils • Continuum of changes (minimal to severe) • Injury occurs within hours of ingestion of gluten • Recovery takes weeks to months, but many never demonstrate improvement • Pathological changes are not pathognomonic
Clinical Features Gastrointestinal Symptoms • Women 20s - 30s, men - slightly later • Diarrhea, abd. distention, flatulence, weakness, lassitude, and weight loss most common • Stools are bulky, loose, pale, float, foul-smelling • Diarrhea usually in morning • Abd. distention and flatulence usually in evening • Abdominal pain is uncommon and may be the first sign of an underlying malignancy
Clinical Features Extraintestinal Symptoms • Anemia (iron, folate, and rarely B12 deficiency) • Poor absorption, sloughing cells, microerosions • Bleeding (vitamin K deficiency) • Osteopenia (bone pain and pathological fractures) • Decreased Ca++ and vitamin D absorption • Intraluminal binding of calcium • Tetany and secondary hyperparathyriodism
Clinical Features Extraintestinal Symptoms • Neurological deficits (hypokalemia and B12 def.) • Paresthesias, sensory deficits, ataxia, peripheral neuropathy • Night blindness (vitamin A deficiency) • Depression and anxiety • Menstrual irregularities and infertility
Physical Findings • Correlates with severity of intestinal involvement • Pallor • Wt. loss, wasting, loose skin folds, hypotension • Cheilosis, glossitis, aphthous ulcers • Doughy, protuberant, tympanic abdomen • Ascites and peripheral edema • Ecchymoses • Hyperkeratosis follicularis • Dec. DTRs or sensation, +Chvostek / Trousseau
Diagnostic Studies Malabsorption Studies • Previously the main diagnostic test • Very nonspecific • Unhelpful in asymptomatic patients • D-xylose test (decrease in serum or urine levels) • Sensitivity = 95% • Lactose intolerance test (inapprop. low glucose) • Breath hydrogen test (inapprop. high expired air hydrogen)
Diagnostic Studies Radiologic Studies • Upper GI barium study • Dilatation of small bowel loops • Coarsening and obliteration of mucosal folds • Nonspecific, thus little use in initial work-up • Irregularly narrowed segments c/w lymphoma • Rigidity c/w collagenous sprue • Osteopenia or pathological fractures on plain films
Diagnostic Studies Serologic Studies • Combination of tests may be adequate for screening high risk individuals • 2% incidence of IgA deficiency • Benefit from treating asymptomatic patients with positive antibody test and characteristic biopsy • Following levels helpful in assessing dietary compliance and disease progression/complications
Diagnostic Studies Histopathologic Studies • Endoscopic duodenal biopsy is the gold standard • Classical histology is not pathognomonic • Second biopsy demonstrating improvement on diet may be replaced by serologic markers • Biopsy (third) after gluten challenge not recommended unless patient is currently on gluten-free diet and initial biopsy not obtained • EGD may show flattening of duodenal folds
Associated Disorders Dermatitis Herpetiformis • 5% of celiac sprue patients have DH • Nearly 100% of DH patients have celiac sprue • Vesicles / excoriations which are pruritic / burning • Associated with HLA-B8 and HLA-Dw3 • Biopsy shows IgA deposits at dermal / epidermal junction • Treatment with gluten-free diet (slow) or dapsone (faster)
Associated Disorders Other Disorders • IgA deficiency - 10 times more frequent • Insulin dependent diabetes mellitus-4.1% have CS • Autoimmune thyroid disease - 4.8% have CS • Sjogren’s syndrome, SLE, vasculitis, RA • IgA mesangial nephropathy • Primary biliary cirrhosis, primary sclerosing cholangitis, inflammatory bowel disease
Treatment and Prognosis • Therapy of choice is lifelong gluten-free diet • Major lifestyle change as common foods have to be substituted / avoided compromising taste • Symptoms improve within days to weeks • Pathological changes take months or longer • Foods may be added back in small amounts (trial) • Most common cause of failed therapy is dietary noncompliance (dietary education is necessary)
Treatment and Prognosis • Those not responding to diet are termed refractory sprue - may respond to corticosteroids • Cyclosporine and azathioprine not proven • Many develop secondary lactase deficiency • Avoid milk products until stable • Replace vitamin and electrolyte deficiencies • Prognosis is excellent for those who respond to a gluten-free diet (majority)
Complications Malignancy • Twofold increase in developing malignancy - lymphoma (50%), carcinoma of esophagus, mouth, pharynx, larynx, and small intestine • Relative risk of lymphoma is 25-120x, greatest in men, older patients, and those untreated >10 years • Suspect when previous diet-responsive patient develops weight loss, abdominal pain, weakness malabsorption, pyrexia, lymphadenopathy
Complications Malignancy • Prognosis poor with surgical resection, XRT, and chemotherapy (9 month life expectancy) • Reason for increased incidence ? • Increased mitotic activity, increased mutations • Increased permeability to carcinogens • Damaged mucosa’s contact with oncoviruses • Strict gluten-free diet reduces risk to 1.2x normal
Complications • Ulcerative Jejunoileitis - 75% mortality • Ulceration and stricture formation - resection • Obstruction, perforation, bleeding, peritonitis • Collagenous Sprue • Subepithelial deposition of collagen • Tend to be refractory - corticosteroid trial • Neurological and Psychological • Sensory ataxia, numbness, tingling, pain, weakness, unsteady gait, depression
Summary • Sm. bowel malabsorptive disease (children/adults) • Intolerance to gluten (wheat, rye, barley, oats) • Abd. discomfort, diarrhea, wt. loss, extraintestinal • Sm. bowel bx (villous atrophy / crypt hyperplasia) • Response to a gluten-free diet (dec. complications) • Serologies aid in screening / following compliance • Prognosis is good as disorder is potentially curable • Potentially fatal disease if overlooked