Download
1 / 25
270 likes | 723 Views
Contraceptive Options for Women and Couples with HIV Injectable Contraceptives. Types of Injectable Contraceptives. Progestin-only. Combined. Hormones. progestin. progestin + estrogen. Duration of effect. 3 months, 2 months. 1 month. Type. DMPA, NET-EN. Cyclofem, Mesigyna.

E N D
Contraceptive Options for Women and Couples with HIVInjectable Contraceptives
Types of Injectable Contraceptives Progestin-only Combined Hormones progestin progestin + estrogen Duration of effect 3 months, 2 months 1 month Type DMPA, NET-EN Cyclofem, Mesigyna
Effectiveness Spermicides Female condom Standard Days Method Male condom Oral contraceptives DMPA IUD (TCu-380A) Rate during perfect use Female sterilization Rate during typical use Implants 0 10 20 25 30 5 15 Percentage of women pregnant in first year of use Source: CCP and WHO, 2007.
DMPA – Mechanism of Action Suppresses hormones responsible for ovulation Thickens cervical mucus to block sperm
DMPA – Most Widely Used Injectable • Best known as Depo-Provera • Used by more than 14 million women worldwide • Administered by deep intramuscular injection • 150 mg every 3 months • Injection site: upper arm or buttocks
Safe Highly effective Easy to use Long acting Reversible Can be discontinuedwithout provider’s help Can be provided outside of clinics Requires no action at time of intercourse Use can be private Has no effect on lactation Has non-contraceptive health benefits Characteristics of DMPA:Advantages
Characteristics DMPA:Non-contraceptive Health Benefits DMPA use may reduce: • Risk of endometrial cancer • Risk of ectopic pregnancy • Risk of symptomatic pelvic inflammatory disease • Uterine fibroids • Frequency and severity of sickle cell crises • Symptoms of endometriosis Source: CCP and WHO, 2007.
Characteristics DMPA:Disadvantages • Causes side effects, particularly menstrual changes • Action cannot be stopped immediately • Causes delay in return to fertility • Provides no protection against STIs/HIV
DMPA – Common Side Effects • Menstrual changes • prolonged or heavy bleeding • irregular bleeding or spotting • amenorrhea (absence of menses) • Weight gain • Headaches, dizziness, changes in mood and sex drive One third of users discontinue during the first year because of side effects. Source: WHO, 1983.
DMPA – Return to Fertility • Does not permanently reduce fertility • Length of time DMPA was used makes no difference • Return to fertility depends on how fast woman fully metabolizes DMPA • on average, it takes 9 to 10 months for women to become pregnant after their last injection Source: Pardthaisong, 1984; Schwallie, 1974.
Infant Exposure to DMPAthrough Breastfeeding • DMPA has no effect on: • onset or duration of lactation • quantity or quality of breast milk • health and development of infant • When to initiate: • after child is 6 weeks old (preferred) Source: Koetsawang, 1987; WHO Task Force for Epidemiological Research on Reproductive Health, 1994; WHO, 2004; updated 2008.
Effect of DMPA on Bone Density • DMPA users have lower bone density than non-users • Women initiating use as adults regain most lost bone • Long-term effect in adolescents unknown • concern that osteoporosis may develop later • long-term studies are needed • generally acceptable to use Source: Cromer, 1996; Cundy, 1994; WHO, 2004; updated 2008.
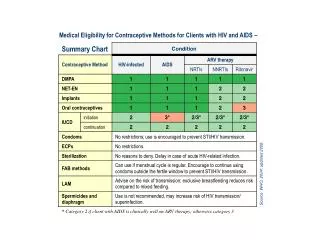
Category 1 and 2 Examples (not inclusive):Who Can Use DMPA WHO Category Conditions Category 1 heavy smokers, breastfeeding after six weeks postpartum, thyroid disorders, severe dysmenorrhea, uterine fibroids, STIs/PID, use of rifampicin or rifabutin, anticonvulsants, or any type of ARV drug ≤18 years, adequately controlled hypertension, uncomplicated diabetes, gall-bladder disease Category 2 Source: WHO, 2004; updated 2008.
Category 3 and 4 Examples (not inclusive):Who Should Not Use DMPA WHO Category Conditions Category 3 breastfeeding before 6 weeks postpartum, severe hypertension (≥160/≥100), vascular disease, acute DVT/PE, current or history of ischemic heart disease or stroke, complicated diabetes, severe liver disease and most liver tumors Category 4 current breast cancer Source: WHO, 2004; updated 2008.
Women with HIV or AIDS can use without restrictions Nevirapine reduces blood progestin level by ~20% DMPA dose provides wide margin of effectiveness On-time injections emphasized Dual method use should be encouraged DMPA Use by Women with HIV Source: WHO, 2004, updated 2008; Mildvan, 2002; Said, 1986.
How to Take DMPA:When to Initiate • Anytime during menstrual cycle if provider is reasonably sure woman is not pregnant • backup recommended if given after day 7 • Postpartum: • not breastfeeding: immediately • breastfeeding: delay 6 weeks • Postabortion: immediately Source: WHO, 2004; updated 2008.
How to Take DMPA:Injection Schedule • Injection every 3 months or 13 weeks • Can be up to 2 weeks early or 4 weeks late Schedule March April June September December Source: WHO, 2004; updated 2008.
Management of DMPA Side Effects:Counseling about Bleeding • Before first injection, counsel that bleeding changes are normal and expected • Provide ongoing counseling and reassurance • If client is concerned or bleeding is severe, treatment or discontinuation may be necessary Counseling is the most important tool for managing bleeding irregularities.
Management of DMPA Side Effects:Treatment of Bleeding • Treatmentoptions • ibuprofen (800 mg three times/day for 5 days) • combined oral contraceptives (COCs) for 21 days • with very heavy bleeding, rule out pregnancy or gynecological problems (uterine evacuation not indicated) Iron supplements can help prevent anemia. Source: CCP and WHO, 2007; WHO, 2004; updated 2008.
Management of DMPA Side Effects:Amenorrhea • Medical treatment not required • If no reason to suspect pregnancy, counsel and reassure that amenorrhea is normal • Pregnancy may need to be ruled out in some cases
Sterile Injection Procedures • Wash hands • Clean injection site • Use sterile needle and syringe • Dispose of waste correctly • Needles and syringes: • single-use must be disposed of safely • reusable must be sterilized
Counseling about DMPA Factors for clients to consider: • Other available contraceptive options • Characteristics (advantages and disadvantages) • Side effects, including menstrual changes • Timing of return to fertility • Need for regular, timely injections
Counseling about DMPA continued ... Messages after choosing DMPA: • Do not massage injection site • Expect bleeding 12–15 days after injection • Return with problems or concerns • No protection from STIs/HIV
Counseling Reduces DMPA Discontinuation • Menstrual changes most common reason for discontinuation • Women receiving appropriate counseling more likely to continue using injectables Source: Lei, 1996.
DMPA – Summary • Safe, effective, easy to use • Nonclinical provision possible • Appropriate counseling essential