Download
1 / 30
410 likes | 989 Views
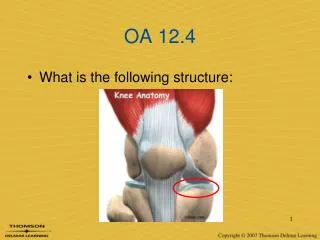
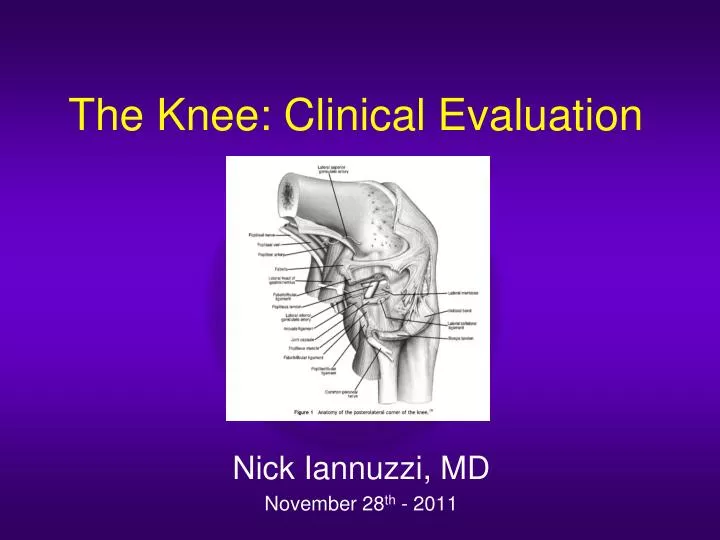
The Knee: Clinical Evaluation . Nick Iannuzzi, MD November 28 th - 2011. Outline. Anatomy History Differential Diagnoses Structured Evaluation Practice Physical Exam. The Knee. The Knee. Exam Maneuvers. Anterior drawer test Lachman test Pivot shift test Posterior sag sign

E N D
The Knee: Clinical Evaluation Nick Iannuzzi, MD November 28th - 2011
Outline • Anatomy • History • Differential Diagnoses • Structured Evaluation • Practice Physical Exam
Exam Maneuvers • Anterior drawer test • Lachman test • Pivot shift test • Posterior sag sign • Posterior drawer test • Quadriceps active test • Valgus stress test • Varus stress test • Patellofemoral grind test • Apprehension test • Joint line tenderness • McMurray Test • Apley grind test • Bounce home test WHAT? WHY? WHEN?
History • Timing? • Mechanism? • Pain description? • Swelling? • Mechanical Symptoms? • Instability? Baker et al 1983; Hughston et al 1985, Laprade et al 1997
Differential Diagnoses • Anterior Knee pain • Extensor mechanism rupture/failure • Patellofemoral pain • Patellofemoral instability • Plica • Arthritis
Differential Diagnoses • Lateral knee pain • Lateral meniscal tear • IT band friction syndrome • Segond fracture • LCL/PLC tear • Gastrocnemius strain/tear • Arthritis
Differential Diagnoses • Medial Knee Pain • Medial meniscus tear • MCL strain/tear • Hamstring strain/tear • Pes anserine bursitis • MPFL disruption • Arthritis
Differential Diagnoses • Posterior knee pain • Popliteal/Baker’s cyst (meniscal tear) • Tumors • Claudication • Radiculopathy
Differential Diagnosis • Locked knee • Meniscal tear • OCD lesion (femur/patella) • Tibial spine avulsion • Osteochondroma (tendons incarcerated)
Rule #1 Always compare to the other Knee!! INTERNAL CONTROL
Inspection/Palpation -Effusion? -Tender? -Skin Breaks? Alignment -Varus/Valgus? -Dislocated? Range of Motion (0-130+) -Mechanical Block -Contractures -Crepitus EXAM-Getting Started WHAT DO YOU SEE?? “Seek Out Disease, Don’t Hope For Health”-anonymous
Inspection/Palpation Alignment Range of Motion (0-130+) Tracking Extensor Mechanism Stability -Provocative Tests GAIT Analysis EXAM-Overview
ACL – Anterior Drawer Knee at 90 degrees Anteriorly translate the tibia with thumbs palpating relationship between femoral condyles and tibia Sensitivity 22-41% (acute injuries); 50-95% (chronic injuries)
ACL - Lachman Exam • Position: -Supine -Knee flexed 0-15 deg • Force Applied:Anterior • Grading Scale: Grade I: 1-5mm Grade II: 6-10mm Grade III: >10mm Sens 80-99%, Spec 95% Gross Anterior Displacement: ACL+PLC Hamstrings Relaxed Feel for Endpoint
ACL - Pivot Shift • Position: -Supine -KneeExtensionFlexion • Force: Valgus, IR • Pathomechanics: -SUBLUXEDReduced -ITT reduces tibia @ 20-30 flexion • Pathoanatomy: -Positive: Glide, Shift, Gross Sens 35-99%, Spec 98% *Key Testable Exam Finding
PCL – Posterior Sag Sign • Position supine • Hip flexed 45 degrees • Knee flexed 90 degrees • Normally, tib plateau extends 1cm beyond femoral condyles • Sens 79%, Spec 100%
PCL - Posterior Drawer • Position: -Supine -Knee flexed 90 deg • Force Applied: Posterior • Pathomechanics: -Post translation tibial plateau -Tibial Plat comp to Femoral Condyle • Pathoanatomy: -G I/IIPCL injury -G IIIPCL + PLC injury Sens 50-100%, Spec 99% Negative in all normal knees, Cooper 1991 Gollehon et al 1987, Grood et al 1988, Noyes 1996
Varus/Valgus Stress • Position: -Supine -Knee 0/30 deg flexion • VALGUS: -0 degMCL + ACL/PCL -30 degMCL • VARUS: -0 degLCL+Cruciate/IT/Bicep -30 degPop/PFL/Lat cap Negative in all normal knees, Cooper 1991
PLC/PCL - ER stress (Dial) • Position: -Prone -Hip Neutral (0 deg flexion) -Knee Flexed 30/90 • Force: ER • Pathomechanics: -Tibial ER on Femur • Pathoanatomy: >10 deg of Asymmetry 30 degPLCInjury 90 degPLC+ PCL Injury TMA-Transmalleolar Axis Negative in all normal knees, Cooper 1991
PLC/PCL - External Rotation Recurvatum • Position: -Supine -Hip neutral (0 deg flexion) -Knee extended • Force: Lift FF anterior • Pathomechanics: -Knee hyperextends -External rotation -Varus • Pathoanatomy: -PLC injury - ±PCL/ACL tear Negative in all normal knees, Cooper 1991
Meniscus – Joint Line Tenderness • Can palpate medial and lateral joint lines of tibia at ~90 degrees flexion • Medial meniscus more prominent with IR • Lateral meniscus more prominent with ER • Sens 55-85%, Spec 30-67%
Meniscus – McMurray’s • Hyperflex knee • Hold heel in one hand • Hold knee with other • Internally rotate knee while extending to 90 degrees • Externally rotate knee while extending to 90 degrees • Can apply varus/valgus stress • Sens 16-58%, Spec 77-98%
Patellofemoral Instability – Q angle • Angle formed by • Line drawn from ASIS to center of patella • Line drawn from center of patella to tibial tubercle • Normal is 10-15 deg
Patellofemoral Instability – Apprehension Sign • Leg hanging off table, supported by thigh • Knee flexed 30 degrees • Attempt lateral translation of patella • Positive sign results when patient flexes quad to resist translation • Sens 39%
Vascular Exam Pulses -Popliteal -DorsalisPedis -Posterior Tibial • Capillary Refill/Warmth Ankle/Brachial Index: ≥0.9 NPV 100% <0.9 PPV 90%, Miranda: 35 knee dislocations Exam :100% NPV ->Popliteal injury -Serial Exams over 24hrs POSITIVE: Angiography or OR!!
KNEE Emergencies? INFECTION DISLOCATION VASCULAR INJURY -Dislocations -Distal femur/Prox Tibia Most knee complaints are NOT emergencies!!
Surgical Problems Pathology Finding ACL Lachmans Meniscus McMurray’s Arthritis Hx/Xray Infection Pain/Effusion/Labs Vascular ABI/Hard Signs
CONCLUSIONS HISTORY EXAMINE NL KNEE R/O EMERGENCY REPETITION IS KEY PHONE A FRIEND IT IS ONLY A VIRTUE IF YOU’RE NOT A SCREWUP!